

Abstract
BACKGROUND: Pulmonary rehabilitation is a key element in the treatment of COPD. Music has been shown to have a positive effect on parameters related to a decrease in exercise tolerance. The aim of this study was to evaluate the effect of listening to ambient music on perceived exertion during a pulmonary rehabilitation session for COPD subjects.
METHODS: COPD subjects randomly performed a session of pulmonary rehabilitation with or without ambient music. Perceived exertion (Borg scales), anxiety (Hospital Anxiety and Depression Scale-Anxiety Subscale), dyspnea (visual analog scale), and cardiorespiratory parameters were compared at the end of both sessions.
RESULTS: Forty-one subjects were analyzed. The characteristics of the COPD subjects were as follows: age, 70.5 ± 8.4 y; body mass index, 22.7 ± 3.9 kg/m2; and FEV1, 38.6 ± 12.5 % predicted. Perceived exertion was not modified by ambient music, but anxiety was improved (P = .02). Dyspnea, fatigue and cardiorespiratory parameters were not influenced by music during a typical session of the pulmonary rehabilitation program.
CONCLUSIONS: This study demonstrates that perceived exertion during one pulmonary rehabilitation session was not influenced by ambient music. However, a positive effect on anxiety was observed. (ClinicalTrials.gov registration NCT01833260.)
Introduction
After initial skepticism, pulmonary rehabilitation has been shown to result in clinically important improvements and effectiveness in patients with COPD. It is an evidence-based, multidisciplinary, and comprehensive program, including exercise training. Its main objectives are reducing symptoms and improving the quality of life and participation in daily life activities of patients. Pulmonary rehabilitation has become a key element in the treatment of patients with COPD. Adherence to exercise training in pulmonary rehabilitation programs is variable and related more to psychosocial than physiological impairment.1,2 It can be negatively influenced by dyspnea, anxiety, and perceived exertion. In 2006, the American Thoracic Society and European Respiratory Society mentioned in their joint statement that all strategies to improve adherence need to be investigated.3
Dyspnea is a subjective breathing discomfort experienced by many patients with COPD4 and results from expiratory flow limitation and lung hyperinflation. Dyspnea is experienced particularly during exercise, resulting in reduced exercise tolerance. Moreover, lower limb muscle dysfunction also contributes to dyspnea during exercise.5 Although previous research explained the physiological mechanisms causing breathlessness in subjects with COPD, dyspnea possesses an important emotional component.
Patients with COPD present with anxiety6,7 and fatigue8 associated with the unpleasant perception of dyspnea and related to various psychological factors.8 Even if there is no evidence of a relationship between failure to complete a rehabilitation program and level of anxiety,9 this last factor is related to reduced exercise tolerance.10 Although anxiety modification is not associated with change in quality of life,11 literature suggests that anxiety can contribute to poor adherence to a pulmonary rehabilitation program.12 The relationship between anxiety and level of daily life physical activities of patients with COPD has not been well evaluated.13
All these components could be positively influenced by distractive auditory stimuli such as music. By analogy, pain perception is improved by focusing attention away from the painful stimulus.14 The effect of music on psychologically modulated factors (mood, emotion, dyspnea) was investigated previously15 and was related to its tempo according to the type of exercise. A slow tempo will benefit an endurance exercise,16 and a fast tempo will improve the work load during exercise.17 Moreover, listening to music was demonstrated to be beneficial in various situations such as during physical exercise,15,18 physiotherapy sessions for subjects with cystic fibrosis,19 and rehabilitation of elderly subjects.20 To our knowledge, its effect was not investigated during a group pulmonary rehabilitation session.
The aim of this study was to evaluate the influence of ambient music on (1) perceived exertion and (2) level of anxiety during a pulmonary rehabilitation session for COPD subjects.
QUICK LOOK
Current knowledge
Distractive auditory stimuli such as music is used in a number of scenarios to reduce the severity of perceived unpleasant procedures. Pain perception appears to be improved by focusing attention away from the painful external stimuli. The impact of distractive auditory stimuli on the sensation of dyspnea has not been studied.
What this paper contributes to our knowledge
The addition of distractive auditory stimuli in the form of music during a session of pulmonary rehabilitation reduced perceived anxiety in a group of subjects with COPD. The effect was immediate, but there was no effect on perceived level of exertion or dyspnea.
Methods
Subjects
Subjects with COPD were recruited from the pulmonary rehabilitation program of Cliniques Universitaires Saint-Luc. To be included, subjects had to participate in the program for at least 1 month after the initial medical investigation in at least 2 of 3 weekly sessions, be free of exacerbations for 1 month, and have maintained exactly the same program session for both evaluated sessions. An exacerbation was defined as follows: “two or more (increased or new-onset) respiratory symptoms such as cough, sputum, wheezing, dyspnea, or chest tightness, lasting at least 3 days, and requiring treatment with antibiotics and/or steroids, and/or hospitalization.”21 Subjects demonstrating rheumatoid pulmonary disease, sarcoidosis, kyphoscoliosis, psychiatric disease, or any musculoskeletal or neurological condition that would limit exercise performance were excluded.
Subjects gave their written informed consent. This study was approved by the institutional medical ethics committee (B403201117655).
Study Design
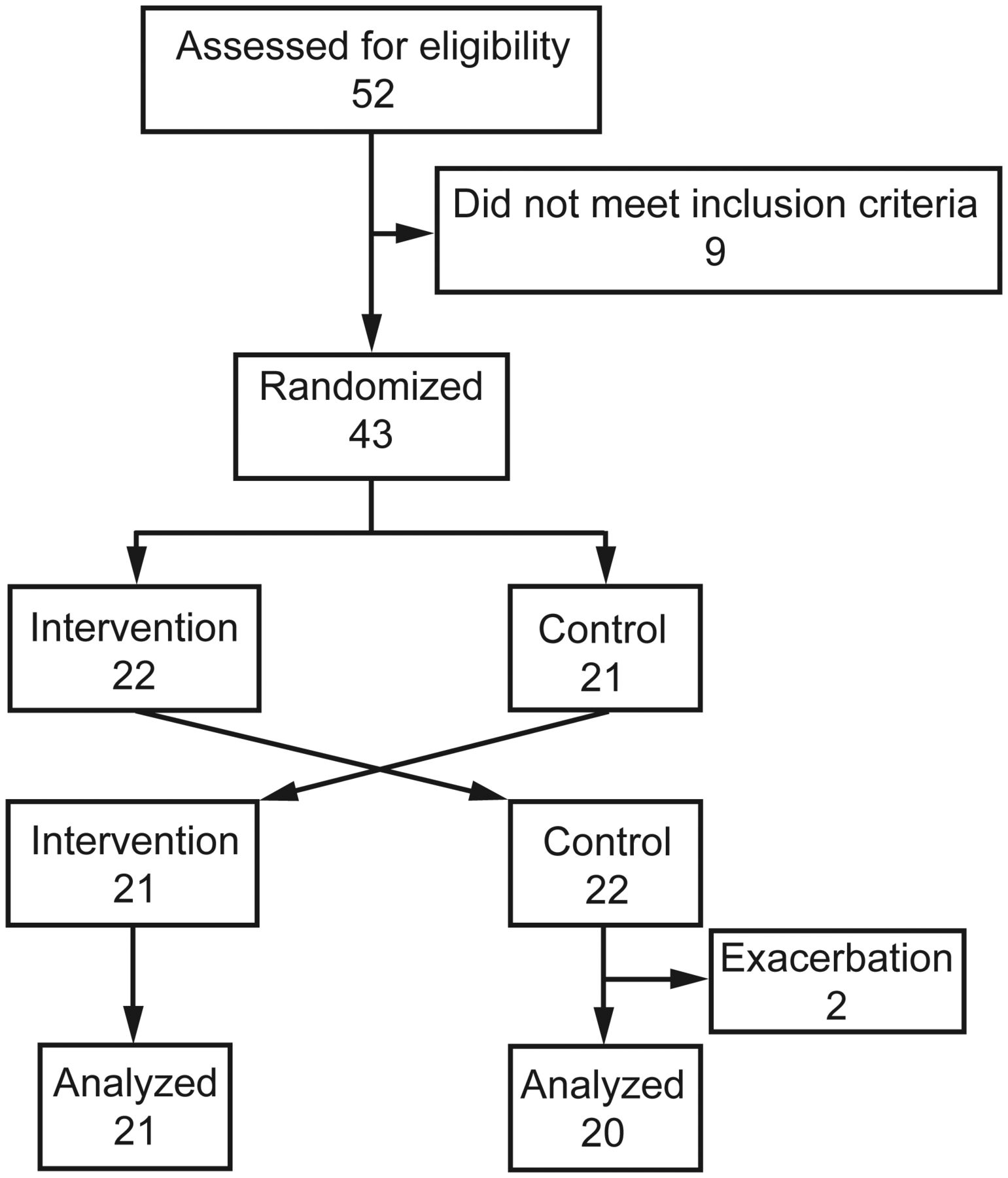
This was a randomized crossover controlled study reported by the Consolidated Standards of Reporting Trials (CONSORT) (Fig. 1). Each subject served as his or her own control and participated randomly in 2 sessions of the pulmonary rehabilitation program under 2 different conditions: with or without a distractive auditory stimulus. The distractive auditory stimulus was a mix of music pieces at the same tempo (120 beats/min). Music was played by 2 speakers in the room at a sound level of 70 decibels (measured in the middle of the room). Randomization of the conditions was performed by a computer-generated random number list. Each subject performed an individualized routine program of exercises next to the other subjects (groups of 20 subjects). The program included aerobic exercise on a cycle ergometer (30 min of interval training: 2 min at 80% of peak power output and 3 min at 50% of peak power output), a rower (endurance for 10 min: fixed intensity based on a visual analog scale score of 5), and a treadmill (based on the average 6-min walk test speed) and strengthening of upper arm and lower leg muscle groups (3 sets of 10 repetitions at intensities of 85% of one repetition maximum). Sessions took place 3 times a week and lasted 1 h and 15 min. Subjects trained at the same load during the 2 consecutive investigated sessions with or without the stimulus depending on its presence during the evaluation session. The interval between the investigated sessions varied from 1 to 6 d.

Flow chart.
Outcomes
Perceived exertion was the main outcome. Heart rate, SpO2, and dyspnea intensity were measured at the beginning and end of each session. At the end of the exercise sessions, perceived exertion, fatigue, anxiety, and satisfaction regarding the session were quantified. Dyspnea intensity was measured by the visual analog scale (from zero [I am not at all short of breath] to 10 [The most short of breath I have ever been]).22 Borg scales were used to rate perceived exertion and fatigue during the sessions.23 Cardiorespiratory parameters (SpO2 and heart rate) were measured by pulse oximetry (Onyx, Nonin, Plymouth, Minnesota). Anxiety was assessed by the Hospital Anxiety and Depression Scale-Anxiety Subscale (HADS-A). Level of satisfaction regarding the session was evaluated by a 10-point Likert scale.
Statistical Analyses
The sample size needed to detect the minimum clinically important difference on the Borg scale4 with a power of 90 was determined (n = 37). Statistical analyses were performed using SPSS Statistics 21.0 (IBM, Armonk, New York). Cardiorespiratory parameters and dyspnea were expressed by the variation between the beginning and end of each session. The difference between the initial and final values was calculated and expressed as a percentage of the initial value (cardiorespiratory parameters) or as an absolute value (dyspnea). Normality of the distributions was verified by the Kolmogorov-Smirnov test. Results are expressed as mean ± SD and CI or as median with interquartile range depending on the normality of the distribution. Results were compared by the paired Student t test. Correlations were analyzed by the Pearson or Spearman correlation coefficient depending on the normality of the distribution. The significance level was set at .05.
Results
The subjects' demographic, anthropometric, and spirometric data are summarized in Table 1. A total of 43 subjects were randomized, and 41 paired sessions were analyzed. Two subjects were excluded due to an exacerbation after the first session. Before each session, heart rate, SpO2, and dyspnea were similar (P > .05) (Table 2). Comparisons of outcomes obtained during sessions with or without music are presented in Tables 2 and 3. The results showed that listening to music during a typical session of a pulmonary rehabilitation program significantly decreased anxiety (P = .02) but did not modify perceived exertion, fatigue, dyspnea, or cardiorespiratory parameters. At the end of the sessions, dyspnea was similar for both conditions (4.9 ± 2.1 and 5.1 ± 2.3, respectively; P = .47).
Demographic, Anthropometric, and Spirometric Data of Subjects With COPD
Outcomes Measured at the Beginning and End of Sessions Performed With and Without Ambient Music
Comparisons of Outcomes Measured During or After Sessions Performed With and Without Ambient Music
When comparing paired sessions (with and without music), HADS-A, visual analog scale, and Borg scales were intercorrelated (Table 4), but there was no relationship for variations in cardiorespiratory parameters or satisfaction.
Correlation Coefficients for Each Outcome Obtained During Sessions With and Without Ambient Music
For both sessions, anxiety was significantly correlated with dyspnea (Fig. 2) but was not correlated with the other cardiorespiratory parameters. Fatigue was significantly correlated with perceived exertion (with music: r = 0.55, P < .001; without music: r = 0.42, P = .006). However, these scales were not correlated with dyspnea at the end of the session.
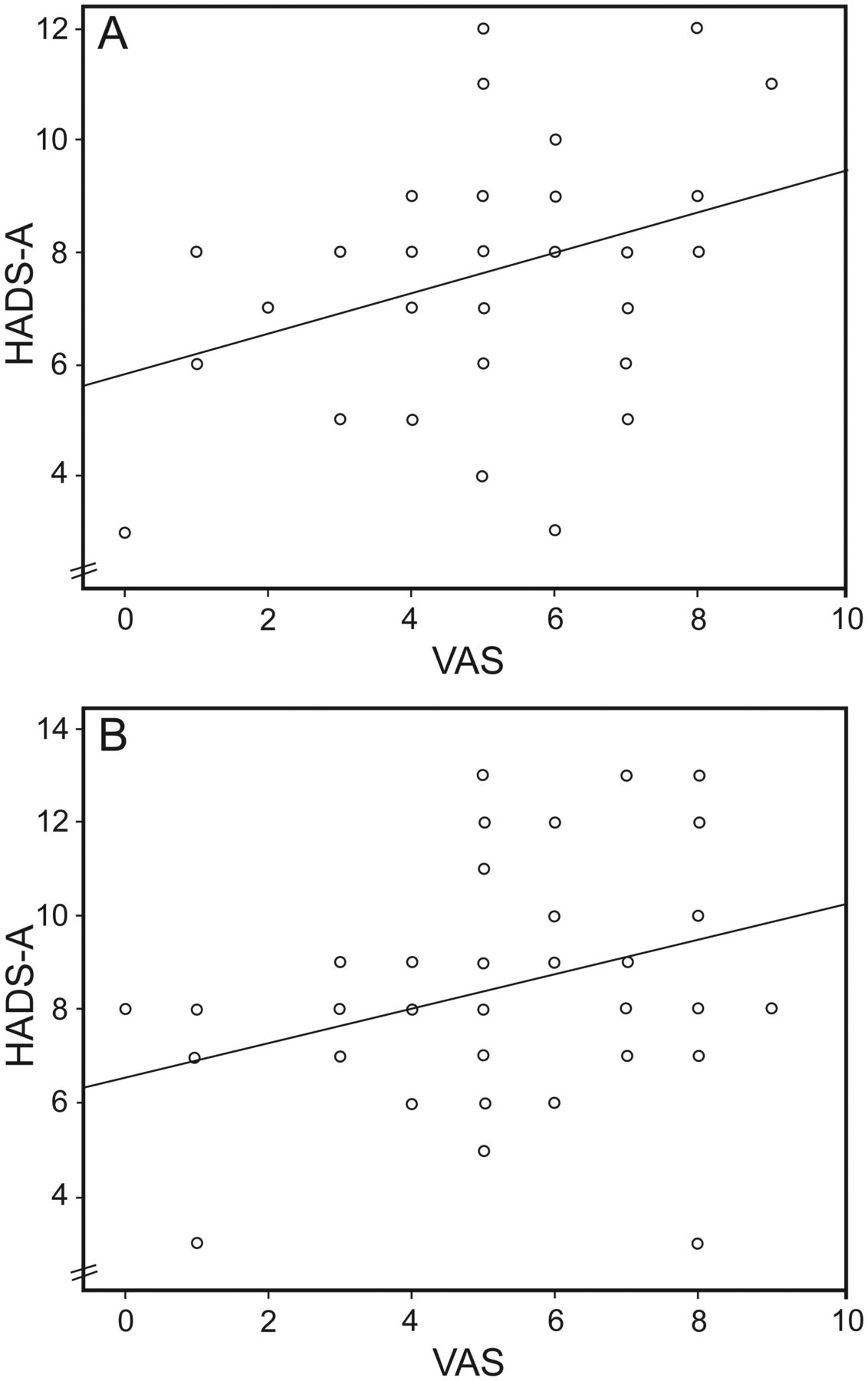
Relationship between anxiety level (Hospital Anxiety and Depression Scale-Anxiety Subscale [HADS-A]) and dyspnea (visual analog scale [VAS]) measured at the end of the sessions. A: with music (r = 0.33, P = .033). B: Without music (r = 0.32, P = .039).
Discussion
To our knowledge, this is the first study to investigate the immediate effect of listening to ambient music during a pulmonary rehabilitation session. The results highlight an improvement in anxiety while listening to music without an effect on perceived exertion in subjects with COPD at the end of the pulmonary rehabilitation sessions. This was shown by an improvement in the HADS-A with a similar Borg scale score between the 2 conditions.
Music was demonstrated to positively influence sensations of endurance and fatigue by distracting subjects.24,25 Moreover, Bauldoff et al26 showed a positive effect of music on dyspnea during performance of daily life activities without modifying anxiety in subjects with COPD. In our study, we noted a decreased anxiety level when subjects listened to music during the exercise sessions. Moreover, a score of >8 points on the HADS-A is considered borderline for anxiety. We found such a mean score in the sessions without music, which was not the case for the sessions with music. The influence of music on anxiety could be considered, depending on the patient's level of anxiety.
Even if exercises are prescribed in the treatment of anxiety disorders,27 in practice, these exercises can generate anxiety due to the exercise limitations of patients with COPD.10 It would be interesting to specify this influence related to the level of training, which is known to modify the anxiety response to exercise,28 and type of music.29 In our population, all subjects had already participated in the program for at least 1 month at the onset of the study, which excluded the influence of training level. The improvement in anxiety could also be related to the motivational environment that music can generate. Such an environment was demonstrated to significantly modify the psychological response with an increase in the stress-responsive hormone cortisol.30
Unlike numerous studies on healthy adults,31–33 athletes,34–36 and subjects with COPD,15,18,37,38 perception of exertion, fatigue, and dyspnea was not influenced by music in our population. The absence of an effect on these parameters is surprising. It could be related to the intensity of the exercise even if the relationship between exercise intensity and benefit of music is not clear for low-to-moderate intensities.15 In our study, exercise intensity was moderate following the pulmonary rehabilitation recommendation that the dyspnea level should not exceed 4–6 on the Borg scale. The mean value was 5 in our subjects at the end of the session. Moreover, dyspnea was significantly intercorrelated between both sessions, suggesting the same exercise intensity for the subjects during the sessions with and without music. The absence of effect on dyspnea is probably related to the measurement of the sensory dimension of dyspnea in our study. Only its affective dimension was demonstrated to be influenced by attentional distraction.39,40
The conditions of the sessions could also explain the absence of a music effect. In contrast to other studies on the effect of music on performance, our subjects were involved in a group program, and music was diffused in the room. When subjects wear headphones, such as in other studies, the distractive phenomenon is probably more important. Another explanation could be related to the style of music. One kind of music is not suitable for all subjects because differences were noted previously depending on personal preferences.41 This hypothesis is reinforced by the absence of a correlation in satisfaction between subjects in both sessions. It highlights the heterogeneity in subject satisfaction. However, the choice of music was shown to have no influence on fatigue perception in healthy subjects.24
The concept of the minimum clinically important difference represents the smallest difference in the outcome of interest perceived by subjects as important and that may lead to a change. It is complementary to the statistical significance. The minimum clinically important difference was determined previously for the visual analog scale (1 cm),42 Borg scale (1 point),43 and HADS-A (1.5 points).44 It is not surprisingly that this difference was not obtained between both sessions. This concept is poorly applicable to the design of our study because it was shown that the minimum clinically important difference for the HADS-A was not reached after a 6-week pulmonary rehabilitation program.45 The minimum clinically important difference is probably more interesting for mid-term or long-term follow-up. It thus seems normal to remain below this level when comparing 2 close sessions as in our protocol.
Exercise tolerance, expressed by variation in heart rate and SpO2 during an exercise training session, was similar in sessions with and without music. In contrast to studies showing a modified heart rate when listening to music during exercises,17 we did not observe this modification. Based on dyspnea, the effort intensity was similar in both sessions. The variations in SpO2 and heart rate during exercise were indeed identical and independent of the auditory stimulus. We did not observe an impact of music on exercise capacity, as was demonstrated previously.38 Our results are similar to those of another study that evaluated the effect of listening to music in subjects with COPD during a 6-min walk test,46 even though exercise duration was different. The design of our study, with a similar level of exercise in both sessions and an evaluation of only one session, did not permit us to observe this influence during a long-term period.
Standardization of methodological conditions is important to avoid some previously demonstrated external influences. Choice of music tempo is important. A tempo of 120 beats/min is the tempo spontaneously adopted by people during an exercise such as walking47 or while performing usual daily activities.48 On a treadmill, this tempo is optimal for slow walking.47 Moreover, it is the more prevalent tempo in a sample of 74,042 pieces of modern music.49 To avoid the demonstrated influence of loudness on treadmill exercise,50 the sound level was fixed for all experiments. Moreover, some uncontrolled factors could have influenced the level of anxiety in our study. Indeed, anxiety symptoms were associated with sleep disturbances in the elderly51 and with mood,52 which could have presented day-to-day variations in our subjects.
Conclusions
In summary, listening to ambient music during a pulmonary rehabilitation session decreased the negative feelings experienced by subjects with COPD and improved anxiety levels. This effect was immediate. However, the level of perceived exertion was not influenced by this short-term intervention. In the future, we will consider introducing music during pulmonary rehabilitation sessions for patients with COPD. However, the benefits of music on a complete pulmonary rehabilitation program need to be evaluated.
Footnotes
- Correspondence: Gregory Reychler PhD PT, Pulmonology Unit, Cliniques Universitaires Saint-Luc, Avenue Hippocrate 10, 1200 Brussels, Belgium. E-mail: gregory.reychler{at}uclouvain.be.
Dr Caty received support from the Institut de Recherche Expérimentale et Clinique, Université Catholique de Louvain. The authors have disclosed no conflicts of interest.
Dr Reychler presented a version of this paper at the 28th Congress of the French Physical Medicine and Rehabilitation Society, held October 17–19, 2013, in Reims, France.
- Copyright © 2015 by Daedalus Enterprises





{kind=link}
{kind=link}