

Abstract
INTRODUCTION: Intubation compromises mucus clearance, allowing secretions to accumulate inside the endotracheal tube (ETT). The purpose of this trial was to evaluate a novel device for ETT cleaning. We hypothesized that its routine use would reduce tube occlusion due to mucus accumulation, while decreasing airway bacterial colonization.
METHODS: Subjects were randomized to either the use of the device every 8 h, or the institutional standard of care (blind tracheal suction) only. ETTs were collected at extubation and analyzed with high-resolution computed tomography (HRCT) for quantification of mucus volume. Microbiological testing was performed on biofilm samples. Vital signs and ventilatory settings were collected at the bedside. In-hospital follow-up was conducted, and a final evaluation survey was completed by respiratory therapists.
RESULTS: Seventy-four subjects expected to remain intubated for longer than 48 h were enrolled (77 ETTs, 37 treatment vs 40 controls). Treated tubes showed reduced mucus accumulation (0.56 ± 0.12 vs 0.71 ± 0.28 mL; P = .004) and reduced occlusion (6.3 ± 1.7 vs 8.9 ± 7.6%; P = .039). The HRCT slice showing the narrowest lumen within each ETT exhibited less occlusion in cleaned tubes (10.6 ± 8.0 vs 17.7 ± 13.4%, 95% CI: 2–12.1; P = .007). Data on microbial colonization showed a trend in the treatment group toward a reduced ETT-based biomass of bacteria known to cause ventilator-associated pneumonia. No adverse events were reported. The staff was satisfied by the overall safety and feasibility of the device.
CONCLUSION: The endOclear is a safe and effective device. It prevents luminal occlusion, thereby better preserving ETT nominal function.
Introduction
The endotracheal tube (ETT) is a life-saving device for respiratory support and airway protection of critically ill patients. However, its sustained presence in the trachea can have harmful consequences by disrupting the physiological mechanisms that maintain mucus homeostasis.1,2
Our group recently studied ETTs collected after discontinuation of mechanical ventilation and showed a significant degree of luminal occlusion, measured by high-resolution computed tomography (HRCT). Similar levels of ETT obstruction were also found in chest CT scans of intubated patients, despite optimal humidification and standard ETT suctioning. The degree of ETT occlusion positively correlated with in vitro measurements of air flow resistance.3 This process of mucus buildup and luminal narrowing leads to an increased ventilatory effort and might delay liberation from the ventilator.4,5 In addition, potential lung pathogens often colonize the ETT lumen.6,7 Bacteria grow as complex biofilms,8 with the plastic surface offering the ideal environment for their proliferation and acquisition of antibiotic resistance.9
Nevertheless, in everyday practice, the extent of ETT biofilm formation and the degree of occlusion are generally not investigated. Despite being poorly effective, blind tracheal suctioning is a standard procedure, commonly used to clear secretions.10,11
Different novel medical devices dedicated to ETT cleaning have recently been developed.12 Among them, we published the successful use of the endOclear® (Endoclear, LLC, Petoskey, Michigan), which we reported to be an effective tool in relieving life-threatening ETT obstruction.13
We hypothesized that the effective removal of secretions would preserve ETT functionality and reduce bacterial lung colonization by preventing luminal occlusion and biofilm formation. We tested this hypothesis in a randomized, controlled clinical trial to assess the efficacy of adding ETT cleaning with the endOclear device to standard ETT maintenance in subjects expected to stay intubated for more than 48 hours. The primary aim of our study was to determine whether tubes treated with the endOclear device (cleaning group) showed an increased luminal patency compared with those receiving only the institutional standard of care (control group). Our secondary aims included: (1) biofilm reduction, (2) improved respiratory mechanics, and (3) safety and feasibility in the use of the device.
QUICK LOOK
Current knowledge
Endotracheal tubes (ETTs) of mechanically ventilated patients may show a significant degree of luminal occlusion due to mucus buildup. Standard tracheal suctioning does not effectively clear secretions, potentially leading to increased air flow resistance and ETT colonization.
What this paper contributes to our knowledge
The implementation of a routine ETT cleaning protocol including the use of the endOclear safely and effectively reduced ETT luminal narrowing.
Methods
Study Setting and Design
The study was conducted across 5 adult intensive care units (ICUs) at the Massachusetts General Hospital (Boston, USA). From March to September 2013, subjects 18 years of age or older were screened twice daily through electronic medical records. Subjects expected to remain on the ventilator for more than 48 hours were enrolled after signed informed consent was obtained from the subject or surrogate. Consented subjects were then randomized through sealed envelopes with a concealed 1:1 allocation to either the treatment or control group. The treatment group consisted of an ETT cleaning protocol involving tracheal suctioning immediately followed by a single pass of the endOclear device, repeated 3 times daily every 8 hours. Subjects in the control group only received the institutional standard of care, which includes blind tracheal suctioning through a closed system (Kimvent, Kimberly Clark, Roswell, Georgia) 3 times a day every 8 hours and as needed. No intervention was planned for control subjects, for whom the study was limited to data collection. The protocol ended at extubation, tracheostomy, or death. Consented subjects requiring re-intubation, re-entered the protocol in the same random group to which they had originally been allocated. Members of the clinical staff and the researchers who supplied the devices and collected data at the bedside were necessarily not blinded to group allocation. However, at extubation, every ETT was assigned an unidentifiable sequential code. Data on ex vivo samples were therefore collected by blinded assessors, particularly GRW and MN for HRCT and LB for microbiology. The study was approved by the Partners HealthCare Institutional Review Board and registered on clinicaltrials.gov (NCT#01765530).
Data Collection
Age, sex, weight, major comorbidities, Simplified Acute Physiology Score (SAPS) II, Acute Physiology and Chronic Health Evaluation (APACHE) II, primary reasons for hospital admission and intubation were recorded at the time of randomization. During the course of enrollment, vital signs and ventilatory settings were recorded at the bedside every 8 hours. For subjects in the treatment group, data were collected twice: before and after the cleaning maneuver. Intubated subjects were connected to either a Puritan Bennet 840 (Covidien, Mansfield, Massachusetts) or Evita 4 (Dräger Medical, Lübeck, Germany) mechanical ventilator with adult size heated-wire ventilator circuits (Hudson RCI-Teleflex, Limerick, Pennsylvania) and active humidification (Neptune, Hudson RCI-Teleflex) at a 37°C set airway temperature, as per institutional practice. At the end of enrollment, electronic medical records were accessed for each patient to establish the incidence of ventilator-associated pneumonia (VAP), as classically defined by clinical, radiological, and laboratory findings.14 In-hospital follow-up was conducted until discharge or death.
The EndOclear Device
The endOclear is a sterile, single-use device consisting of a proximal handle, and a thin flexible catheter with a cleaning apparatus at its terminal end (Fig. 1). A distal rounded-tip mesh structure can be mechanically activated to move from a collapsed to a radially expanded position. During use, the catheter is first inserted into the ETT. Once in position, the device is activated to form a disc-shaped wiper that gently presses upon the ETT inner wall. The endOclear is then withdrawn from the tube over a period of 3–5 seconds, scraping secretions off the inner ETT wall. For safety purposes, the device is equipped with graduated markings and an adjustable safety guide to help prevent over insertion. A safety lock at the handle level averts untimed triggering of the device. Along with the device, a Y-shaped connector is supplied by the manufacturer. This connector allows mechanical ventilation to be continued during the maneuver and secretions to be collected in a disposable, dedicated adapter. The endOclear device is marketed as a Class 1 FDA 510(k) exempt device.

A schematic representation of the endOclear device. A: A full view of the device, from the handle, to the central tube (45.7 cm, size 3.2 mm), to the cleaning apparatus. Note the red safety toggle and the blue stop, which can be positioned on the appropriate centimeter marking to avoid over-insertion. B: Insertion of the endOclear into an endotracheal tube. Detailed view of device activation from the collapsed (C) to radially-expanded configuration (D). The wiper disc diameter expands from 4.5 mm to approximately 9.4 mm once deployed. Secretions are cleared from the endotracheal tube lumen by withdrawing the expanded device.
Endotracheal Tube Processing
ETTs were collected at the bedside immediately after extubation, sealed, and rapidly processed for further analysis (see the supplementary materials at http://www.rcjournal.com for a schematic overview of the ETT processing protocol from the moment of patient's extubation). Every effort was undertaken to reduce as much as possible the time needed to complete every step. Specifically, we aimed at limiting possible alterations of the endoluminal content occurring after extubation, to avoid imaging artifacts and bacterial contamination. A detailed report of the time lapses between the different steps of our protocol is provided in the supplementary materials at http://www.rcjournal.com.
High-Resolution Computed Tomography Scanning
HRCT was obtained for the terminal 22 cm end of each ETT, as already described elsewhere.3 Raw imaging data of mucus and air volumes (mL) were acquired and subsequently converted to volume percentages (mucus/[mucus+air], % mL). We, therefore, report as “overall occlusion” the average ratio of mucus versus total ETT inner volume (mucus+air) throughout the whole 22 cm tube portion. HRCT data were then analyzed slice-by-slice, to identify the single point of maximum volume occlusion within each ETT, which we refer to as “maximum occlusion” (% mL). Once the slice showing the highest occlusion was identified, further computation of imaging data was performed to calculate the lowest cross-sectional area (CSA, mm2) available to air flow throughout the ETT. Approximating such CSA to that of a circle, the lowest “mucus-free” internal diameter (ID, mm) was estimated for each tube in the 2 groups. We refer to this last parameter as minimum ID. Graphical schematization of our HRCT spatial analysis is provided in Figure 2.

A: High-resolution computed tomography (HRCT) spatial analysis. The endotracheal tube was first analyzed as a whole to collect data about the total mucus volume (mL), and the overall occlusion % (total mucus/(mucus + air)). The single slice showing the highest degree of luminal narrowing was also identified and studied to detect the maximum occlusion % (B). Assuming uniform mucus distribution, its measured cross-sectional area (CSA; cm2) was then approximated to that of a circle (C), in order to estimate the endotracheal tube lumen actually available to airflow (minimum internal diameter, mm =  ). The Murphy-eye and the beveled edge of the tip of the endotracheal tube (terminal 16mm) were excluded from HRCT analysis due to the incompletely circular cross-section, causing artifacts in the volumetric computation. Sample representative HRCT mid-sagittal (D) and transversal (E) endotracheal tube scans are also shown. CSA = cross-sectional area.
). The Murphy-eye and the beveled edge of the tip of the endotracheal tube (terminal 16mm) were excluded from HRCT analysis due to the incompletely circular cross-section, causing artifacts in the volumetric computation. Sample representative HRCT mid-sagittal (D) and transversal (E) endotracheal tube scans are also shown. CSA = cross-sectional area.
Microbiology
Collection of mucus samples and ETT standard microbiological testing were performed as previously described.3 Routine identification and quantitation of bacterial and fungal isolates were obtained from each collected ETT. Resistance to major antibiotics was also tested. The impact of cleaning on ETT bacterial biofilm was analyzed by grouping isolates into 4 major categories (No Growth, Pathogens, VAP-causative Gram Negatives,15 and Multi-Drug-Resistant16).
Safety and Staff Feedback
At the end of the trial, a standardized questionnaire was administered to registered respiratory therapists (RRTs) to collect their feedback on the use of the endOclear. Users were asked to grade the device on a scale from 1 (poor) to 4 (excellent), regarding its efficacy in cleaning the ETT, its safety, and its usability. An overall evaluation was finally requested on a scale from 1 to 10. Respiratory therapists were instructed to promptly notify the research staff in case of any adverse event, defined as an untoward, accidental, and unfavorable circumstance temporarily associated with the cleaning maneuver and to that at least partially attributable, with or without harm being caused to the patient (eg, device malfunction or breakage, accidental extubation, tracheal injury).
Statistical Analysis
The primary end point of the study was the difference in overall ETT occlusion between the 2 groups. We hypothesized an average 2 ± 1 mL less mucus, as an effect of the cleaning device in the treatment arm. Based on preliminary HRCT data, we anticipated enrolling a total of 74 subjects in a randomized-controlled design (37 subjects per group) to detect this difference for a statistical power of 80%, with a 2-sided significance level of 0.05 in a 2-sample t test. Further details about the conducted power analysis are provided in the supplementary materials at http://www.rcjournal.com.
Normal distribution of each tested variable was assessed with the Shapiro-Wilk test. Data are reported as mean ± standard deviation (SD) or median [interquartile range, IQR], as appropriate. Differences between the 2 groups were tested with the Student t test or Wilcoxon rank-sum test based on distribution normality. Ratios and proportions between groups were compared using the chi-square test. A P < .05 was considered statistically significant.
The analysis was conducted with Stata 12.0 (Stata Corporation, College Station, Texas) and Prism 6 (GraphPad, La Jolla, California) software.
Results
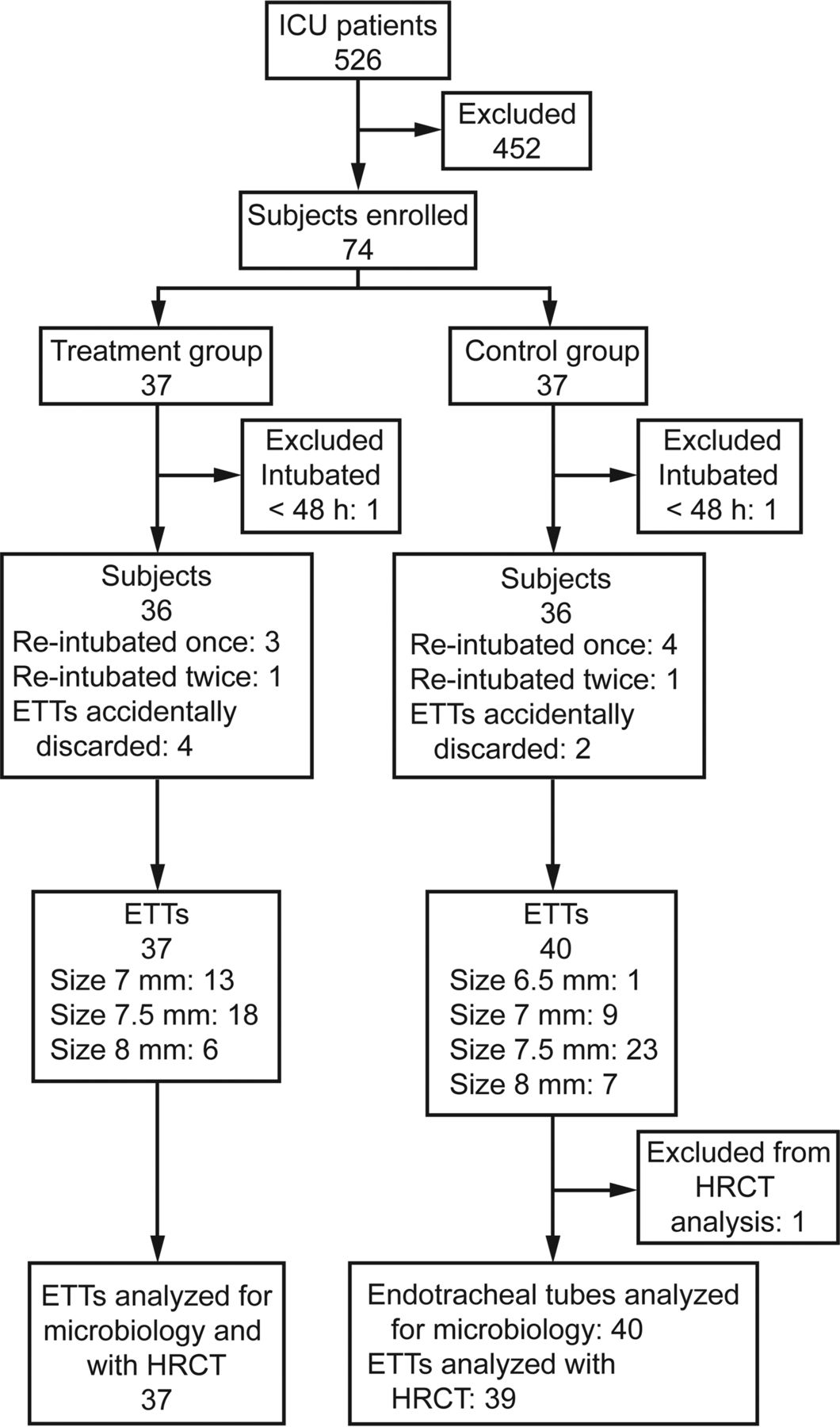
A total of 526 intubated subjects were screened to enroll 74 subjects, subsequently randomized 37 versus 37 to the treatment and control groups. One subject in each group was excluded due to intubation lasting fewer than 48 hours. Seven subjects were reintubated once (3 treatment vs 2 control), while one subject per group was reintubated twice. Six ETTs were accidentally discarded at extubation (4 treatment vs 2 control), giving a total of 37 and 40 tubes collected in the cleaning and control groups, respectively (Fig. 3).
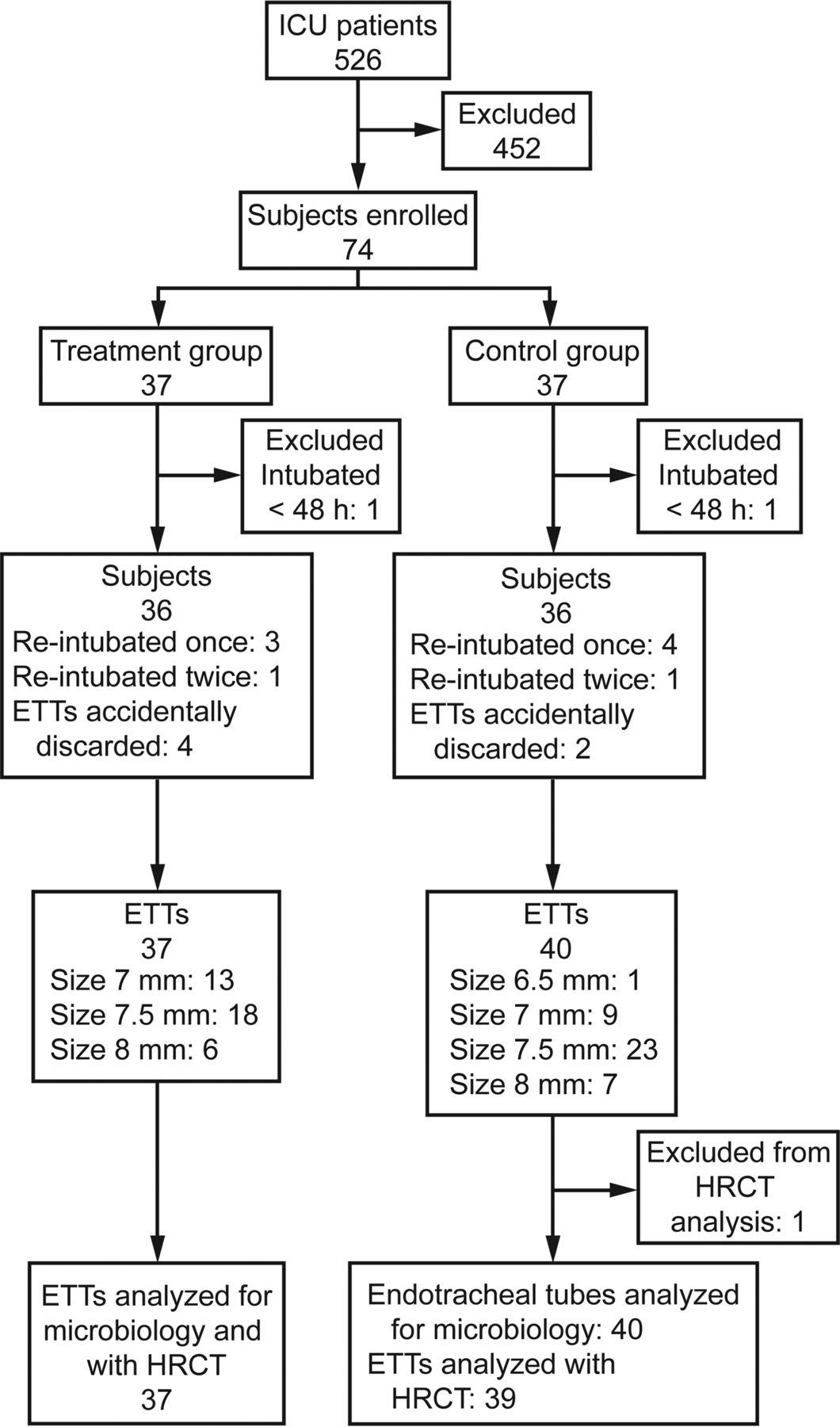
Flow chart. ETT = endotracheal tube, HRCT = high-resolution computed tomography.
Baseline characteristics of the study population are shown in Table 1. No significant differences between the 2 study groups were recorded at baseline. Specifics of the different ETTs collected throughout the study are provided in the supplementary materials at http://www.rcjournal.com.
Study Population and Baseline Characteristics
High-resolution Computed Tomography (Table 2)
HRCT Data
Endotracheal tubes cleaned with the endOclear device every 8 hours as a supplement to the standard of care showed reduced mucus accumulation (Mucus Volume: 0.56 ± 0.12 mL vs 0.71 ± 0.28 mL, treatment vs control, P = .004). A significant difference was also recorded after normalization of mucus for the total luminal volume (overall occlusion: 6.3 ± 1.7% vs 8.9 ± 7.6%, P = .039; Fig. 4). The HRCT slice of each tube showing the narrowest lumen exhibited significantly less occlusion in tubes treated with the device (maximum occlusion: 10.6 ± 8.0% vs 17.7 ± 13.4%, P = .007). ETTs from both groups showed variable degrees of ID reduction compared with their nominal size. In the most numerous subgroup of size 7.5 mm ETTs, the minimum ID was significantly wider in the cleaning group (7.2 [7.0–7.3] mm vs 7.0 [6.5–7.1] mm, P = .001). No differences were recorded for 7.0 and 8.0 mm tubes. The ratio of ETT occlusion did not correlate with the length of intubation, as shown in the supplementary materials at http://www.rcjournal.com. A single 6.5 mm tube (control group) was excluded from HRCT analysis due to size discrepancy.

Slice-by-slice mean luminal occlusion due to mucus accumulation along scanned endotracheal tubes (ETT) from lung (0 cm) to oral (22 cm) end. Data from 0 to 1.6 cm are intentionally omitted as described in the Methods section.
Microbiology (Table 3)
Colonization of Collected ETTs by Bacterial and Candida Species
The isolation frequency of pathogenic bacteria in mucus retrieved from collected ETTs did not differ between the 2 groups. No difference was recorded in terms of antibiotic susceptibility patterns. Notably, the use of the device was associated with a 6-fold increase in the probability of finding ETTs for which no bacteria at all were isolated. Also, known VAP-causative gram-negative organisms (GN) were 50% less likely to be found in cleaned ETTs than in controls. However, these trends did not reach statistical significance (Relative Risk [95% CI], No growth: 6.49 [0.81–51.36], P = .07; gram-negative VAP-causatives: 0.50 [0.23–1.1], P = .08).
Vital Signs and Respiratory Parameters
Data collected 3 times daily at the bedside were grouped into 4 main time-points (study d-1, d-3, d-5, and d-7). Further details about recorded ventilatory settings and the effect of cleaning on ventilatory parameters can be found in the supplementary materials at http://www.rcjournal.com.
Safety and Staff Feedback
In-hospital follow-up was completed for all subjects. No adverse events occurred throughout a total of 584 cleaning procedures. Completed questionnaires from a total 28 RRTs were collected: 25/28 users (82%) considered the endOclear to be “much better” (grade 4) or “better” (grade 3) than standard suctioning. Ease of setup was also positively evaluated, and the device's overall assigned score was 7.1 ± 2.1. Please refer to the supplementary materials at http://www.rcjournal.com for a detailed description of follow-up data and a full report of the user survey.
Discussion
This randomized, controlled clinical trial evaluated the efficacy of a device specifically designed to clean the endotracheal tube lumen of airway secretions. We showed that tubes treated with the endOclear were significantly less occluded than controls, as measured by HRCT.
Narrowing of the endotracheal tube due to secretions is usually an underestimated problem.17 Mucus attached to the inner ETT surface reduces the volume available to air flow,5 thereby leading to increased airway resistance18 and patient's work of breathing (WOB).4 In some cases, the gradual luminal narrowing can progress to complete occlusion of the ETT. In prior studies,19,20 the degree of ETT occlusion was estimated by using acoustic reflectometry and averaged between 10% and 15%. This noninvasive technique indirectly estimates the tube cross-sectional area (CSA), by analysis of sound waves as they propagate throughout the tube. Our group developed and reported on an innovative methodology for the analysis of ETT occlusion based on HRCT imaging.21 We detected an average 25% CSA reduction, compared with paired control unused tubes. Imaging data correlated with in vitro measurements of resistance. Moreover, a variable degree of mucus partially occluding the ETT could also be visualized on standard chest CT scans.3 Compared with acoustic reflectometry, our novel assay based on HRCT offers several advantages, including: (1) the direct visualization and quantitation of mucus volume, and (2) a precise definition of the mucus accumulation pattern across the whole ETT length.
Currently, blind suctioning through a small flexible catheter is the most common method to remove secretions from within the ETT.22 This maneuver can injure the tracheal mucosa,23 decrease lung volume leading to hypoxia,24 trigger cardiac arrhythmias,25 and increase intracranial pressure.26 In addition, the use of blind suctioning has also been associated with further impairment of tracheal mucociliary clearance function27 together with dislodging emboli of pathogens from the ETT biofilm to the lower airway.28 Several novel dedicated medical devices have been developed for the specific purpose of ETT cleaning. Different from suctioning, the aim of these devices is to remove mucus by physically scraping the inner wall of the tube. Among this new generation of cleaning catheters, we found the endOclear to be a safe and effective device in the clinical setting.13 Its efficacy, however, had never been tested in a randomized, controlled fashion.
According to our HRCT results, the use of the endOclear device led to a reduced amount of mucus attached to the inner wall of the ETT after extubation. Consequently, tubes in the treatment group had reduced occlusion. Wright et al demonstrated that the ETT alone significantly contributes to total air flow resistance.29 Luminal narrowing due to mucus accumulation further increases resistance, which varies inversely to the fourth power of the tube's radius, according to the Poiseulle equation:
 where ΔP is the pressure drop, L is the length of the conduit, μ is the fluid viscosity, Q is the flow, and r is the radius. An increased air flow resistance due to luminal narrowing significantly adds to subjects' WOB, as shown in vivo by Heyer et al.30 According to the authors' estimate, a 10% reduction in the ETT cross-sectional area would correspond to a 27% increase in a patient's WOB.30 Subjects receiving pressure-support ventilation, especially if awake and/or during weaning protocols, might considerably benefit from the reduced respiratory load otherwise imposed by accumulated secretions.
where ΔP is the pressure drop, L is the length of the conduit, μ is the fluid viscosity, Q is the flow, and r is the radius. An increased air flow resistance due to luminal narrowing significantly adds to subjects' WOB, as shown in vivo by Heyer et al.30 According to the authors' estimate, a 10% reduction in the ETT cross-sectional area would correspond to a 27% increase in a patient's WOB.30 Subjects receiving pressure-support ventilation, especially if awake and/or during weaning protocols, might considerably benefit from the reduced respiratory load otherwise imposed by accumulated secretions.
Conti et al31 tested an “obstruction remover” in 8 mechanically ventilated subjects, showing a significant reduction of in vivo airway resistance, as well as a reduced WOB. In 2003, the Mucus Shaver was developed by Kolobow et al.32 This device, although not commercially available, was shown to be effective in clearing secretions from the ETT first in an animal study,32 followed by a small clinical trial.33 More recently, Liu et al34 investigated the use of 8F sterile urinary catheters as an easily available alternative to the Shaver in a population of 45 intubated children. Similar to the Shaver, the regular implementation of this ETT cleaning maneuver reduced bacterial colonization and biofilm thickness as determined by confocal microscopy. However, none of these devices are commercially available, and all of these studies lacked accurate measurements of ETT patency.
In our study, we also tested the hypothesis that, by mechanically scraping the ETT inner surface, the use of the endOclear could interfere with the process of biofilm formation, therefore delaying colonization by clinically relevant pathogens. To test this secondary end point, we categorized bacterial isolates as “VAP causatives,” according to a retrospective analysis of VAP microbial etiology conducted at our institution.15 In this work by Arvanitis et al, 208 VAP cases over a 5-y period were identified by searching a large hospital infection control database (approximately 40 VAP cases/year). Nevertheless, we did not find any significant difference in the rate of ETT colonization between the 2 groups. Among our selected population of intubated subjects, we registered a total of only 7 clinically diagnosed VAP cases over 6 months. Focusing on the ETT microbial colonization by Gram-negative VAP-causative agents, we isolated such bacteria in 7 treated ETTs versus 15 controls, meaning a 50% relative reduction in the risk of isolating such pathogens in cleaned tubes. However, it is likely that this trend did not reach statistical significance due to the small sample size. Alternatively, the use of a cleaning device might not be effective by itself in limiting the process of biofilm formation. We are currently exploring whether there is a synergic effect between ETT cleaning with the endOclear and the use of an antibacterial coating on the ETT lumen to reduce biofilm formation in the ETT (ClinicalTrials.gov NCT#02120001).
Throughout our study enrollment, the endOclear was safely used, with no adverse events reported over several ETT cleaning maneuvers. However, albeit unlikely, ETT displacement and tracheal injury must still be considered as potential risks associated with the use of the device. We believe the careful application of the available safety measures (red toggle, centimeter markings, blue safety stop) will significantly reduce the likelihood of such complications.
This study has several limitations. First, the enrollment design did not control ETT size. Ideally, to avoid any confounding factors, enrolled subjects should have been intubated with same-sized, same-brand tubes, or at least a size-balanced randomization should have been implemented. Second, in a trial involving 5 heterogeneous ICUs, no unit-based randomization was planned to limit possible confounders related to the type of admission. However, despite a slight imbalance in subjects being intubated due to respiratory failure, no significant baseline differences were recorded between the 2 groups. Third, no blinding of the respiratory therapists performing the study treatment could physically be applied, potentially leading to a bias due to the staff being more scrupulous when using the new device compared with usual care. Fourth, our study protocol did not include any restrictions on the institutional practice for tracheal suctioning. The aim of the study was to test the efficacy of routine ETT cleaning with a dedicated device in addition to the standard of care. However, a different rate of suctioning between the groups, although unlikely, could have altered our findings. Finally, this is a phase 2 randomized clinical trial to establish the effectiveness of cleaning of the lumen of the ETT; therefore, no conclusions can be drawn regarding major clinical outcomes.
Larger studies are needed in order to establish the role of ETT cleaning in terms of reducing time on the ventilator, length of ICU stay, and VAP incidence. Additionally, technical features must be developed and tested to improve the functionality of cleaning devices and promote their routine use. At our institution, the use of the endOclear was adequately implemented with no adverse events reported, and the respiratory therapists involved in the protocol positively reviewed the device. The endOclear is a first-generation product that still requires disconnection of the patient from the mechanical ventilator. A promising solution would be to implement such cleaning apparatus on a closed suction system, to avoid repeated disruptions of the breathing circuit.
Conclusions
In our trial, ETT luminal narrowing was safely and effectively reduced by the implementation of a routine cleaning protocol, which included the use of a dedicated device. The subsequently increased tube patency might be beneficial to critically ill mechanically ventilated patients. Larger studies are needed to test whether this translates to improved clinical outcomes.
Acknowledgments
Eleftherios Mylonakis MD PhD (Rhode Island Hospital and The Miriam Hospital, Warren Alpert Medical School of Brown University, Providence, Rhode Island) for his help in the study design and review of microbiological data.
Francesco Nordio PhD (Brigham and Women's Hospital, Boston, Massachusetts) for statistical consultation and review.
Medical student Dominique Monlezun for his assistance in the processing of study samples and data collection.
Mary Delaney, Andrea Dubois, Rose Deng, and Qing Liu (Center for Clinical and Translational Metagenomics, Brigham & Women's Hospital, Boston, Massachusetts) for microbiological samples processing.
Jessica Truelove, BS, Benoit Tricot, MS, and the Center for System Biology-Mouse Imaging Program at the Massachusetts General Hospital (Boston, Massachusetts) for their help with HRCT scanning and imaging analysis.
The Nursing and Respiratory Therapy staff of the Massachusetts General Hospital-Critical Care Center (Boston, Massachusetts).
Footnotes
- Correspondence: Lorenzo Berra MD, Department of Anesthesia, Critical Care and Pain Medicine, Massachusetts General Hospital. White 434-B, 55 Fruit Street, Boston, Massachusetts 02114. E-mail: lberra{at}mgh.harvard.edu.
Dr Mietto presented a version of this paper at the 43rd Critical Care Congress of the Society of Critical Care Medicine 2014, held January 9–13, 2015, in San Francisco, California.
Supplementary material related to this paper is available at http://www.rcjournal.com.
This study was funded in part by the Department of Anesthesia, Critical Care and Pain Medicine, Department of Respiratory Care, Massachusetts General Hospital. Endoclear, LLC supported microbiological testing, HRCT analysis, and supplied the endOclear devices free of charge. Microbiological testing at the Center for Clinical and Translational Metagenomics was partially funded by NIDKK P30DK034854. Dr Kacmarek is a consultant for Covidien, has received honararium (1 per y) for a lecture by Maquet and has received a grant from Venner Medical. None of the other authors has any conflict of interest to disclose.
See the Related Editorial on Page 1560
- Copyright © 2016 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}