

Abstract
BACKGROUND: Lung ultrasound is increasingly becoming a diagnostic tool in the critical care setting. B-pattern on a lung ultrasound is an artifact composed of multiple B-lines and correlates with interstitial edema. A randomized controlled trial concluded that bedside thoracic ultrasound could predict postextubation distress through changes in lung aeration during a weaning procedure; however, it could not screen patients before performance of a spontaneous breathing trial (SBT).
METHODS: We conducted a 2-year, prospective, multicenter, observational study in 2 adult medical-surgical ICUs in southern Brazil. All enrolled subjects met eligibility criteria for ventilation liberation. Patients with tracheostomy were excluded. Lung ultrasound was performed immediately before SBT. B-predominance was defined as any profile with anterior bilateral B-pattern. The primary outcome was SBT failure, defined as the inability to tolerate a T-piece trial of 30–120 min, in which case subjects were not extubated.
RESULTS: From 2011 to 2013, 250 subjects undergoing weaning procedures were evaluated. SBT failure occurred in 51 (20.4%) subjects. Subjects with a successful SBT were extubated on the first attempt in 75.6% of cases. B-predominance was a very weak predictor for SBT outcome, showing 47% sensitivity, 64% specificity, 25% positive predictive value, and 82% negative predictive value.
CONCLUSION: B-pattern detected by a simplified lung ultrasound protocol should not preclude hemodynamically stable, sufficiently oxygenated patients from performing an SBT.
Introduction
Liberation from mechanical ventilation remains one of the most challenging aspects of caring for critically ill patients. Clinical trials from the 1990s clearly showed that clinicians frequently did not appreciate that ventilator withdrawal was possible in a timely fashion.1,2 Although lifesaving as long as needed, continuing mechanical ventilation is associated with increased morbidity and mortality, varying with age, the severity of preexisting and current disease processes, and ventilator plus interface (endotracheal or tracheostomy)–associated complications.3,4 On the other hand, failed or unplanned extubation is followed by marked clinical deterioration, suggesting a direct and specific effect of extubation failure and re-intubation on patient outcomes.5 The clinical challenge then is to balance aggressiveness with safety.6,7
Lung ultrasound has several advantages over conventional radiological means for assessing lung abnormalities in that it is reliable and accurate, highly reproducible, noninvasive, and easily repeatable at the bedside.8,9 B-lines are vertical hyperechoic sonographic artifacts that arise from the pleural line, extend to the bottom of the screen without fading, move synchronously with lung sliding, and erase A-lines. The presence or absence of B-lines is a useful tool for identifying pulmonary edema and alveolar interstitial syndrome in the acute setting, and there is evidence of real-time matching of B-line quantity with changes in extravascular lung water and total body water.10–15 Correlation between pulmonary artery occlusion pressure and B-lines in critically ill patients suggests it is a useful surrogate of left-sided filling pressures.12,16,17
Weaning-induced cardiac dysfunction is recognized as an important cause of weaning failure.18–20 Switching a patient from positive-pressure ventilation to spontaneous breathing reestablishes negative inspiratory intrathoracic pressure, thus increasing venous return (left ventricular preload), central blood volume, and left ventricular afterload.18,19 Increases in extravascular lung water induced by spontaneous breathing trials (SBTs) were detected in individuals who eventually failed weaning.21
In the last 20 years, from physiology to epidemiology, it seems that every imaginable factor with any potential to influence patients' ability to recover spontaneous breathing has been studied, and a large body of sometimes contradictory evidence has led to very different conclusions.22–24 One case report assessing both global and regional lung de-recruitment provided useful insights into the etiology of weaning failure.25 Soummer et al26 demonstrated that progressive lung de-recruitment during an SBT may accurately identify patients likely to fail extubation. However, as far as we know, no study has addressed the potential role of lung ultrasound findings in identifying individuals who are likely to fail to wean, so that either premature unsuccessful SBTs or undesirable delays could be avoided. Indeed, it is often unclear which factors should be considered in the decision-making process. Our previous study lacked sufficient power to detect any significant effects.27 Therefore, we sought to assess prospectively whether B-pattern of congestion seen on lung ultrasound prior to initiation of an SBT correlated with weaning outcomes in a heterogeneous group of mechanically ventilated subjects.
QUICK LOOK
Current knowledge
Bedside lung ultrasound is a notable diagnostic tool in the ICU setting. B-lines are the sonographic sign for detecting pulmonary edema. Given the predictable negative physiological effects of pulmonary edema and large pleural effusions on lung mechanics, it is reasonable to consider whether checking for B-line predominance on lung ultrasound might be helpful to optimize the patient's condition before a spontaneous breathing trial (SBT) to increase the likelihood of successful extubation.
What this paper contributes to our knowledge
In 250 ready-to-wean individuals who underwent lung ultrasound immediately before an SBT, visualization of B-pattern bilaterally on the anterior chest performed poorly in predicting SBT failure. Lung ultrasound findings of B-predominance on a simplified 4-zone protocol should not interfere with the decision to initiate weaning procedures, as it does not identify individuals who will fail an SBT.
Methods
Between January 2011 and March 2013, nonconsecutive subjects ≥ 18 y old who had undergone invasive mechanical ventilation for 24 h were enrolled from 2 medical-surgical ICUs in private hospitals in southern Brazil. Individuals with a tracheostomy were excluded. The research ethics board at each center approved the study and waived the requirement for informed consent. The study was registered as NCT02022839 at http://clinicaltrials.gov.
Subjects were assessed daily for eligibility to wean according to current guidelines, which included improvement of underlying condition that led to acute respiratory failure; alert and able to communicate; adequate gas exchange, as indicated by an arterial pressure of oxygen of at least 60 mm Hg with an FIO2 < 0.40; no significant respiratory acidosis; rapid shallow breathing index ≤ 105 breaths/min/L; and vasoactive drugs at low and stable doses (norepinephrine doses < 0.12 μg/kg/min or equivalent dopamine doses).28,29 While local weaning protocols at both sites did not standardize PEEP levels as a prerequisite, it is a common practice to keep it < 8 cm H2O before starting a T-piece trial.
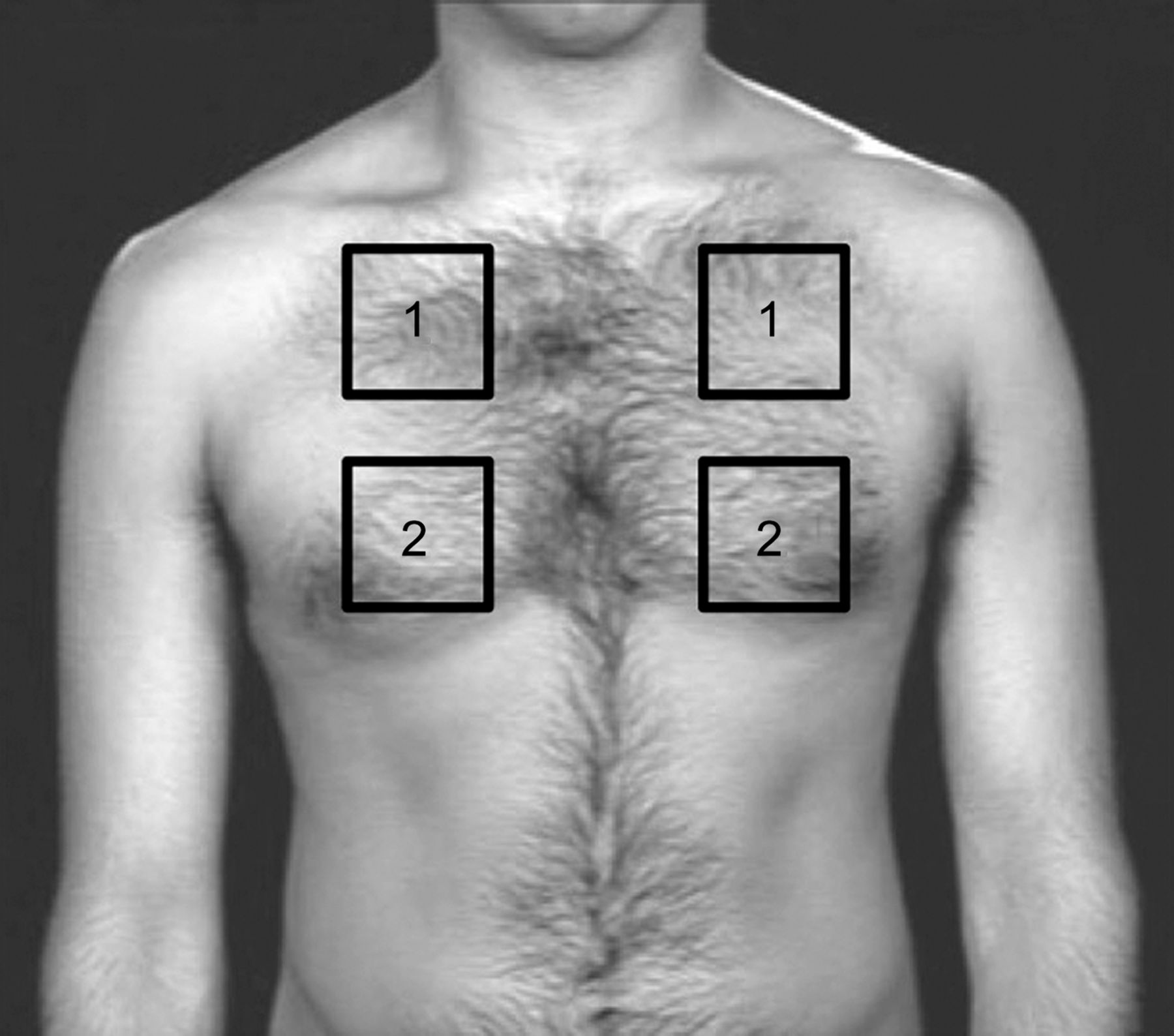
A trained investigator using a 2- to 4-MHz convex probe performed lung ultrasounds as previously described.9,10,12,30 Subjects were scanned while in a semi-recumbent or supine position, immediately before starting the SBT. We divided the anterior thoracic surface into 4 areas, corresponding to the intercostal spaces between the third and fourth ribs and between the sixth and seventh ribs; the probe was inserted at the center of each, making 4 points of investigation per lung with dichotomous answer, requiring < 1 min (Fig. 1). Any profile with anterior bilateral B-pattern was denoted as B-predominance, which defines interstitial syndrome.9 We did not describe patterns of aeration other than A-line, B-line, and C-line; the number of single or confluent B-lines was not reported.

The 4 parasternal views corresponding to the intercostal spaces between the third and fourth ribs and between the sixth and seventh ribs used to investigate B-pattern.
The main outcome of interest was SBT failure, defined as an inability to tolerate a T-piece SBT of 30–120 min, in which case subjects were not extubated. The breathing trial was interrupted if subjects developed signs of respiratory discomfort (frequency > 35 breaths/min, arterial oxyhemoglobin saturation < 90%, use of accessory respiratory muscles or paradoxical thoracoabdominal ventilation), tachycardia (heart rate > 140 beats/min), hemodynamic instability (systolic blood pressure < 90 mm Hg or 20% over baseline levels), or change in mental status (drowsiness, coma, anxiety).29 There were no secondary end points for this study.
Demographic data including age, gender, race, comorbidities, severity of illness at the time of ICU admission, reason for the initiation of mechanical ventilation, physiological weaning predictors, and fluid balance (total inputs minus total outputs) in the 48 h preceding the SBT were recorded. The presence of diastolic or systolic left ventricular dysfunction (the latter condition defined as ejection fraction < 45%) was documented according to a formal echocardiogram report dated up to 6 months prior to admission. Diagnosis of COPD was based on history, physical examination, chest radiograph, and previous pulmonary function tests, if available.
Statistics
Results were expressed as the mean ± SD, median (interquartile range), or proportions, as appropriate. The normal distribution of the various parameters was investigated using the Kolmogorov-Smirnov test. We used the Student t test or the Mann-Whitney U test to compare continuous variables, and the chi-square test or the Fisher exact test to compare proportions, as appropriate. Sensitivity, specificity, positive predictive value, negative predictive value, positive likelihood ratio, and negative likelihood ratio of B-predominance for the prediction of SBT failure were calculated. A P value < .05 was considered statistically significant. Statistical analysis was performed with SPSS v.20.0 (SPSS, Chicago, Illinois).
Results
We obtained complete data in 250 subjects undergoing weaning procedures. Overall, failed SBT occurred in 51 (20.4%) cases. Table 1 shows the baseline characteristics of the study cohort according to outcome. One hundred and eighty-nine individuals (75.6%) were extubated on the first attempt - i.e., simple weaning procedures. Subjects who were successfully extubated were older (median 75 vs 66 y, P = .03) and had been intubated for a shorter duration (median 4 vs 7 d, P < .001). There was also a lower prevalence of COPD in the SBT success group (19.6% vs 9.5%, P = .045).
Characteristics of the Study Cohort
B-predominance was observed in 95 cases, but only 24 subsequently failed SBT. Likewise, 27 subjects who did not succeed on SBT had showed no bilateral B-pattern prior to the T-piece SBT. B-predominance was a very weak predictor for SBT failure, as it provided sensitivity, specificity, positive predictive values, and negative predictive values of 0.47 (95% CI 0.33–0.61), 0.64 (95% CI 0.57–0.70), 0.25 (95% CI 0.17–0.35), and 0.82 (95% CI 0.75–0.88), respectively.
Contrary to what was expected, individuals who exhibited B-predominance also had lower fluid balance in the 48 h prior to weaning procedure (966 [1,167.7–3,050] mL vs 1,588 [100–3,100] mL, P = .043), possibly by chance. The large variability of values is shown in Figure 2.

Range of values of fluid balance in the preceding 48 h of spontaneous breathing trials according to finding of B-predominance on lung ultrasound. Median (range) fluid balance was lower in the B-predominance group, although there was a wide range of values: 966 (1,167.7–3,050) mL vs 1,588 (100–3,100) mL, P = .043.
Discussion
In a heterogeneous cohort of mechanically ventilated weaning candidates, the lung ultrasound finding of B-predominance on a simplified 4-zone protocol did not have the potential to alter decisions to start an SBT. Our data suggest that incorporating an ultrasonographic estimation of lung edema in the readiness criteria for withdrawal of mechanical ventilation potentially delays the decision.
The myriad changes in respiratory mechanics and cardiovascular status related to weaning failure do not become evident until clinical manifestations of distress, which promptly demand test interruption or re-intubation.31 Delaying SBT until B-lines wane (due to the belief that individuals could not pass a T-piece trial until they were dry again) has the potential to delay the overall weaning process. B-line artifacts may also be affected by other dynamic changes, such as the application of PEEP and the respiratory cycle,32 and we could not demonstrate any correlation between higher fluid balance and B-predominance. Fluid balance values did not predict SBT outcomes in a medical-surgical ICU population, and using pleural drainage to accelerate liberation from mechanical ventilation is also not supported by evidence.33,34
While we were in the process of gathering data for this study, Soummer et al26 reported that a quantitative assessment of 6 chest regions with lung ultrasound accurately predicted extubation failure by identifying global and regional lung derecruitment at the end of SBT. They speculated that subjects who eventually required re-intubation had either greater tendency to pulmonary collapse or lack of muscle endurance. However, the authors were unable to anticipate 14 individuals who failed on a 60-min T-piece trial and thus were not extubated; lung ultrasound scores before SBTs were not different between groups.26
In a preliminary report,27 we postulated that a simplified approach using 4 anterior chest zones would be adequate for the specific purpose of our study because the B-pattern or consolidation found at lower and posterior lung regions was likely to indicate gravitational changes. Such a 4-zone protocol has been successfully adopted for other purposes elsewhere.10,13,16,35 Indeed, reducing scanning to just 4 anterior chest zones facilitated initial assessment of this subset of subjects through a simple, inexpensive, safe, rapid, and easy-to-perform screening test.9,10,30 Within up to 1 min of lung ultrasound examination, researchers were able to reliably identify B-pattern. The counting approach may be imprecise when considering single scanning sites, and although it has utility as a research tool, it may be overly complicated for the front-line intensivist to use in a busy ICU. No conclusions could be drawn regarding more precise quantification of interstitial syndrome and the relationship to SBT outcomes using different protocols, such as an 8-, 12-, or even a 28-zone approach.
We chose SBT failure as the principal outcome because we aimed to predict the earliest time that a patient might resume spontaneous breathing. Moreover, the exact reason for extubation failure often escapes identification. Re-intubation is usually performed because of an apparently new episode of respiratory distress, which may be related to primary respiratory failure, congestive heart failure, aspiration, ineffective cough with airway secretion build-up, upper airway obstruction, onset of new sepsis, surgical complications, acute coronary syndrome, or neurological impairment. This multiplicity of causative factors explain persistent uncertainties about the pathophysiology of extubation failure.31
Limitations of our study were its observational design, its intrinsic methodological flaws, and its small sample size. Lung ultrasound examinations were performed only during working hours. The choice of a convenience sample also limits the interpretation and generalization of the findings. The prevalence of simple weaning (75.6%) indicates that our prospective opportunity sample had same expected pre-test probability of SBT failure as any ordinary, medical-surgical ICU population.28,29,31 Simple weaning was defined as proceeding from initiation of weaning to successful extubation on the first attempt without difficulty.28 No echocardiographic data were obtained; however, because increases in respiratory load and cardiac load are strongly interrelated, it is difficult to estimate the real incidence of cardiac-related weaning failure.18,19 Neither transthoracic echocardiogram changes nor brain natriuretic peptide levels provided clinically useful cutoffs for predicting postextubation distress in a previous study.26 Only 24 (9.6%) of subjects included in our study had a history of cardiac failure, thus no inference could be made. Like all ultrasound techniques, bedside lung-ultrasound quality can be operator-dependent; however, a high intra- and inter-observer reproducibility has been reported.36
One may wonder whether it is really pertinent to predict results of a simple and safe test such as an SBT rather than to simply perform it. There is no definitive evidence that a carefully monitored but unsuccessful SBT is detrimental to weaning outcome. To the contrary, in a study of 1,067 subjects undergoing daily screens, only a one major complication (0.1%) could be possibly attributed to a failed SBT.37 Therefore, in our opinion, there is no real need to perform lung ultrasound simply to avoid proceeding to an SBT in individuals already meeting eligibility criteria for weaning.
Conclusion
The B-pattern detected by a simplified lung ultrasound protocol should not preclude hemodynamically stable and sufficiently oxygenated patients from performing an SBT. Likelihood ratios are not high enough to serve as standalone criteria for clinical decision making. Lung ultrasounds may be helpful in defining a mechanism for weaning failure and in guiding intervention that may increase the success of the next attempt, particularly when integrated with echocardiography. A multicenter, randomized, interventional study is required to assess the impact of an ultrasound algorithm on weaning rate, length of stay, and ICU mortality.
Footnotes
- Correspondence: Ana Carolina P Antonio MD PhD, 910 Ramiro Barcelos, 3rd floor Porto Alegre, Brazil. E-mail: ana.carolina.antonio{at}gmail.com
Dr Antonio presented a version of this paper at the 25th ESICM Annual Congress held October 13–17, 2012, in Lisbon, Portugal.
The authors have disclosed no conflicts of interest.
- Copyright © 2018 by Daedalus Enterprises





{kind=link}
{kind=link}