

Abstract
BACKGROUND: The use of noninvasive ventilation in patients with left-ventricular dysfunction may increase cardiac performance by decreasing inspiratory effort and left-ventricular afterload. The aim of the present study was to evaluate the acute effects of noninvasive ventilation on central-venous oxygen saturation (Scv̄O2) and blood lactate in subjects with left-ventricular dysfunction during the early postoperative phase of coronary artery bypass grafting.
METHODS: This study included 100 subjects during the postoperative phase of elective coronary artery bypass grafting. Blood samples, at 5 time points, were collected to assess tissue perfusion markers (ie, Scv̄O2 and blood lactate) as follows: (1) the intraoperative period (after anesthesia induction); (2) 20 min after ICU arrival, under intermittent mandatory ventilation; (3) 20 min after extubation with spontaneous breathing; (4) after 1 h of noninvasive ventilation; and (5) 20 min after discontinuation of noninvasive ventilation.
RESULTS: A significant increase in the blood lactate and a drop in the Scv̄O2 were observed on arrival to the ICU compared with intraoperative values (P < .001). After extubation, during spontaneous breathing, the Scv̄O2 significantly decreased (P = .02), whereas the blood lactate increased, although not significantly (P = .21) compared with intermittent mandatory ventilation on arrival to the ICU. During the application of noninvasive ventilation, the Scv̄O2 significantly increased (P = .048) and the blood lactate significantly decreased (P = .008) compared with spontaneous breathing values after extubation. After noninvasive ventilation discontinuation, the Scv̄O2 and blood lactate did not change compared with measures taken during noninvasive ventilation; higher values of Scv̄O2 were maintained compared with those obtained after extubation (P < .001).
CONCLUSIONS: The acute application of noninvasive ventilation improved Scv̄O2 and decreased the blood lactate in subjects with left-ventricular dysfunction during the early postoperative phase after coronary artery bypass grafting. (ClinicalTrials.gov registration NCT02767687.)
- cardiac surgery
- central-venous oxygen saturation
- arterial lactate
- noninvasive ventilation
- tissue perfusion
- left-ventricular dysfunction
- coronary artery bypass grafting
Introduction
Coronary artery bypass graft surgery, when properly indicated, is a clinical standard of care that decreases mortality and can contribute to improved quality of life; this is particularly the case in those patients with left-ventricular (LV) dysfunction.1 However, postoperative complications, such as acute renal failure, septic shock, and systemic acute inflammation, are associated with tissue hypoxia. Central-venous oxygen saturation (Scv̄O2) and blood lactate are accepted markers of tissue oxygenation and independent predictors of morbidity and mortality after coronary artery bypass graft surgery.2
Previous studies that assessed cohorts of subjects who underwent cardiac surgery demonstrated that Scv̄O2 and blood lactate are associated with short- and long-term clinical outcomes, including 5-y survival.2–4 Importantly, patients with LV dysfunction may continue to experience a deterioration in myocardial function after surgery, which leads to a worsening mismatch between supply and demand of oxygen, which is detected by a low Scv̄O2 and an elevated blood lactate.3
A previous study reported that a decline in Scv̄O2 could be augmented during early postsurgical mobilization (ie, the first or second day after cardiac surgery), attributed to a reduction in the compensatory cardiac response with physical movement.5 In this scenario, resuscitation strategies involve goal-directed therapy to enhance preload, afterload, and contractility to match metabolic demand and reverse global tissue hypoxia.6
There is evidence that the use of noninvasive ventilation (NIV) in subjects with LV dysfunction may increase cardiac performance by decreasing inspiratory effort and LV afterload.7–9 Currently, there is a gap in the literature with regard to whether NIV, through an improvement in cardiac performance, is able to increase tissue perfusion in patients with LV dysfunction after coronary artery bypass graft surgery. Therefore, the aim of the present study was to evaluate the acute effects of NIV on Scv̄O2 and arterial blood lactate in subjects with LV dysfunction during the early postoperative phase after coronary artery bypass graft surgery.
QUICK LOOK
Current knowledge
Central-venous oxygen saturation (Scv̄O2) and blood lactate are important independent predictors of morbidity and mortality after cardiac surgery. Positive results after noninvasive ventilation (NIV) application in patients with left-ventricular (LV) dysfunction may be due to its capability to improve cardiac performance by decreasing inspiratory effort and LV afterload. Currently, the literature remains unclear as to whether NIV, through an improvement in cardiac performance, is able to increase tissue perfusion in subjects with LV dysfunction after coronary artery bypass grafting.
What this paper contributes to our knowledge
NIV provided improvement on tissue perfusion markers in subjects during the postoperative period of coronary artery bypass graft surgery; this was expressed by an increase in Scv̄O2 and a decrease in the blood lactate. To the best of our knowledge, this was the first study that evaluated the acute NIV effects in tissue perfusion specifically in subjects with LV dysfunction during the early postoperative period of cardiac surgery.
Methods
The current study was conducted at the cardiac surgery ICU of the São Paulo Hospital of the Federal University of São Paulo. All subjects signed an informed consent form before study enrollment. The study took place from June 2015 to August 2016 and was approved by the institutional ethics committee.
Subjects
Male and female patients who had elective coronary artery bypass graft surgery were eligible for the current study. Inclusion criteria consisted age 35–75 y at the time of surgery, a history of LV dysfunction with an LV ejection fraction of ≤ 0.45, and admission under intermittent mandatory ventilation in the ICU. A diagnosis of COPD, morbid obesity, neurologic disease, hemodynamic instability, an emergency surgery indication, extubation in the operating room, extubation after 24 h of invasive ventilation, NIV intolerance, or extubation failure served as exclusion criteria.
Surgical Procedures
Anesthetic procedures were conducted in a routine fashion with midazolam and maintained with sufentanil and isoflurane (0.5–1%). The subjects underwent a standard invasive ventilation protocol in volume control continuous mandatory ventilation with a tidal volume (VT) of 8 mL/kg of predicted body weight, PEEP of 8 cm H2O, breathing frequency to maintain PaCO2 between 35 and 45 mm Hg, and FIO2 sufficient to maintain oxygen saturation > 90%.
The operation was performed through a median sternotomy by using the left internal thoracic artery, complemented with additional saphenous vein grafts. After systemic heparinization to keep activated coagulation time > 480 s, the on-pump technique was established with ascending aorta cannulation and single cannula venous drainage. Myocardial protection was achieved by using intermittent hypothermic antegrade blood cardioplegia associated with systemic mild hypothermia (34°C). The off-pump technique (off-pump coronary artery bypass grafting) was performed with the aid of an Octopus 3 (Medtronic, Minneapolis, Minnesota) suction stabilizer, and, to maintain normothermia, a heated water mattress was used throughout the operation. Before chest closure, in the presence of an incidental left pleura opening, a soft tubular polyvinyl chloride drain was inserted and exteriorized at the subxiphoid region and was positioned in the left costophrenic sinus. A straight mediastinal drain was also placed via a tubular subxiphoid in all the subjects.
Postoperative Management
After the surgical procedure, all the subjects were transferred to the cardiac surgical ICU. While the subjects were under intermittent mandatory ventilation, they were ventilated with volume control continuous mandatory ventilation with a VT of 6–8 mL/kg of predicted body weight, PEEP of 10 cm H2O, and FIO2 of 0.4. Extubation was performed according to an established ICU protocol, and, afterward, a 40% air-entrainment mask was used for 20 min. Sequentially, NIV was delivered via an orofacial interface by using a Servo-s mechanical ventilator (Maquet, Rastatt, Germany), with bi-level positive airway pressure (pressure support and PEEP) for 1 h. Inspiratory pressure was adjusted to maintain a VT of 6–8 mL/kg of predicted body weight, PEEP of 10 cm H2O, and FIO2 of 0.4. After NIV application, the subjects were returned to a 40% air-entrainment mask for 20 min. The same analgesic protocol was administered with 100 mg of tramadol hydrochloride 3 times a day.
Study Design
In the early postoperative period, blood samples were collected to assess tissue perfusion status. Blood samples for Scv̄O2 analysis were obtained from a central-venous catheter, and blood samples for arterial blood lactate and arterial oxygen saturation (SaO2) were obtained from a standard catheter inserted into the radial artery. Blood samples were collected at 5 time points: (1) the intraoperative period after anesthesia induction; (2) 20 min after ICU arrival during intermittent mandatory ventilation, adjusted according to the aforementioned standard protocol; (3) 20 min after extubation in spontaneous breathing with a 40% air-entrainment mask; (4) after 1 h of NIV immediately before NIV removal; and (5) 20 min after NIV discontinuation with a 40% air-entrainment mask. Moreover, during these 5 time points, the arteriovenous oxygen content difference (C(a-v)O2) was calculated as a measurement of tissue oxygen extraction (ie, the difference in oxygen content between arterial and venous blood).10
Statistical Analysis
Categorical data were expressed in absolute (n) and relative (%) frequency. Semicontinuous and continuous variables were expressed as mean ± SD. Variables were tested for normality distribution by applying the Kolmogorov-Smirnov test. One-way analysis of variance for repeated measures with the Tukey post hoc test was performed to analyze tissue perfusion markers at different time points for each subject. The 2-way analysis of variance with the Tukey post hoc test was performed to analyze the variables from the subjects who either underwent on-pump or off-pump coronary artery bypass graft surgery at different time points. A P < .05 was considered statistically significant for all tests. Statistical analyses were performed by using GraphPad Prism 7.0 software (GraphPad Software, La Jolla, California).
Results
One hundred forty-eight patients were eligible for the current study; 48 were excluded, as illustrated in Figure 1. Clinical and demographic characteristics are described in Table 1.

Flow chart. NIV = noninvasive ventilation.
Clinical and Demographic Characteristics of the Subjects
A significant increase in blood lactate and a drop in Scv̄O2 were observed on arrival to the ICU in comparison with intraoperative values (after anesthetic) (P < .001). After extubation, while spontaneously breathing, compared with admission when the subjects were invasively ventilated, Scv̄O2 significantly decreased (P = .02) and arterial blood lactate increased, although not significantly (P = .21) (Fig. 2).
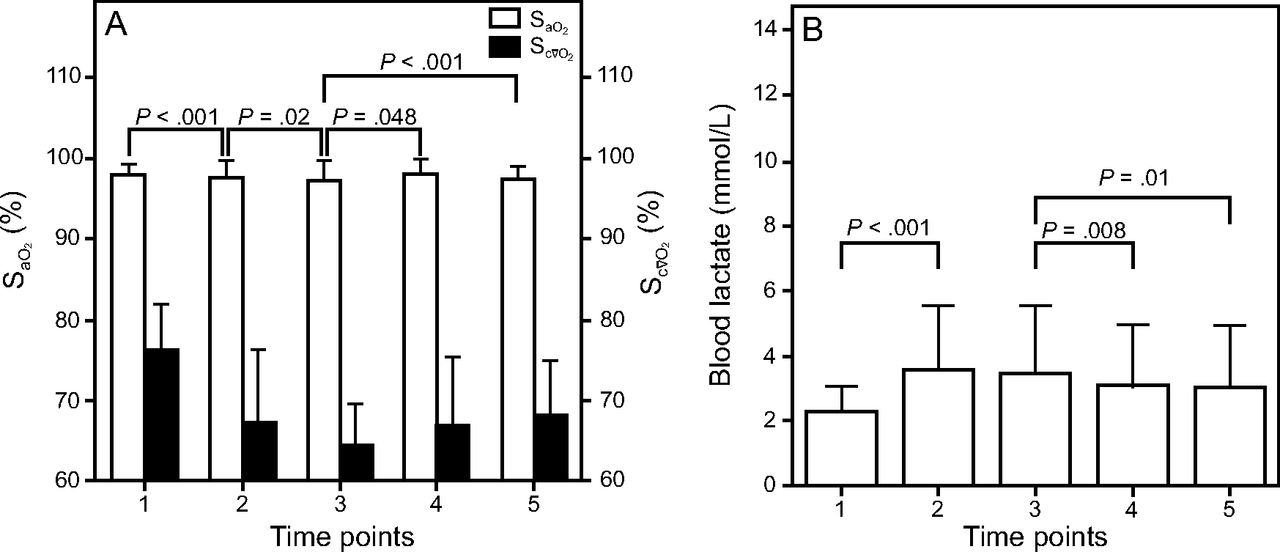
Sequential changes of central-venous oxygen saturation (Scv̄O2) and arterial oxygen saturation (SaO2) (A) and blood lactate (B) at 5 time points to assess (1) the intraoperative period (after anesthesia induction), (2) 20 min after arrival to the ICU (under intermittent mandatory ventilation), (3) 20 min after extubation in spontaneous breathing, (4) after 1 h of noninvasive ventilation (NIV) (immediately before NIV removal), and (5) 20 min after NIV discontinuation. Values are given as mean ± SD.
During NIV application, Scv̄O2 significantly increased (6.34% increase; P = .048) (Fig. 2A) and blood lactate showed a significant decrease (11.77% decrease, P = .008) (Fig. 2B) compared with spontaneous breathing values before NIV. At 20 min after NIV discontinuation, the Scv̄O2 was not different when compared with NIV application and maintained greater values compared with the postextubation time before NIV (P < .001) (Fig. 2A). The blood lactate was not different when compared with the time of NIV application and maintained lower values compared with the blood lactate before NIV (P = .01) (Fig. 2B).
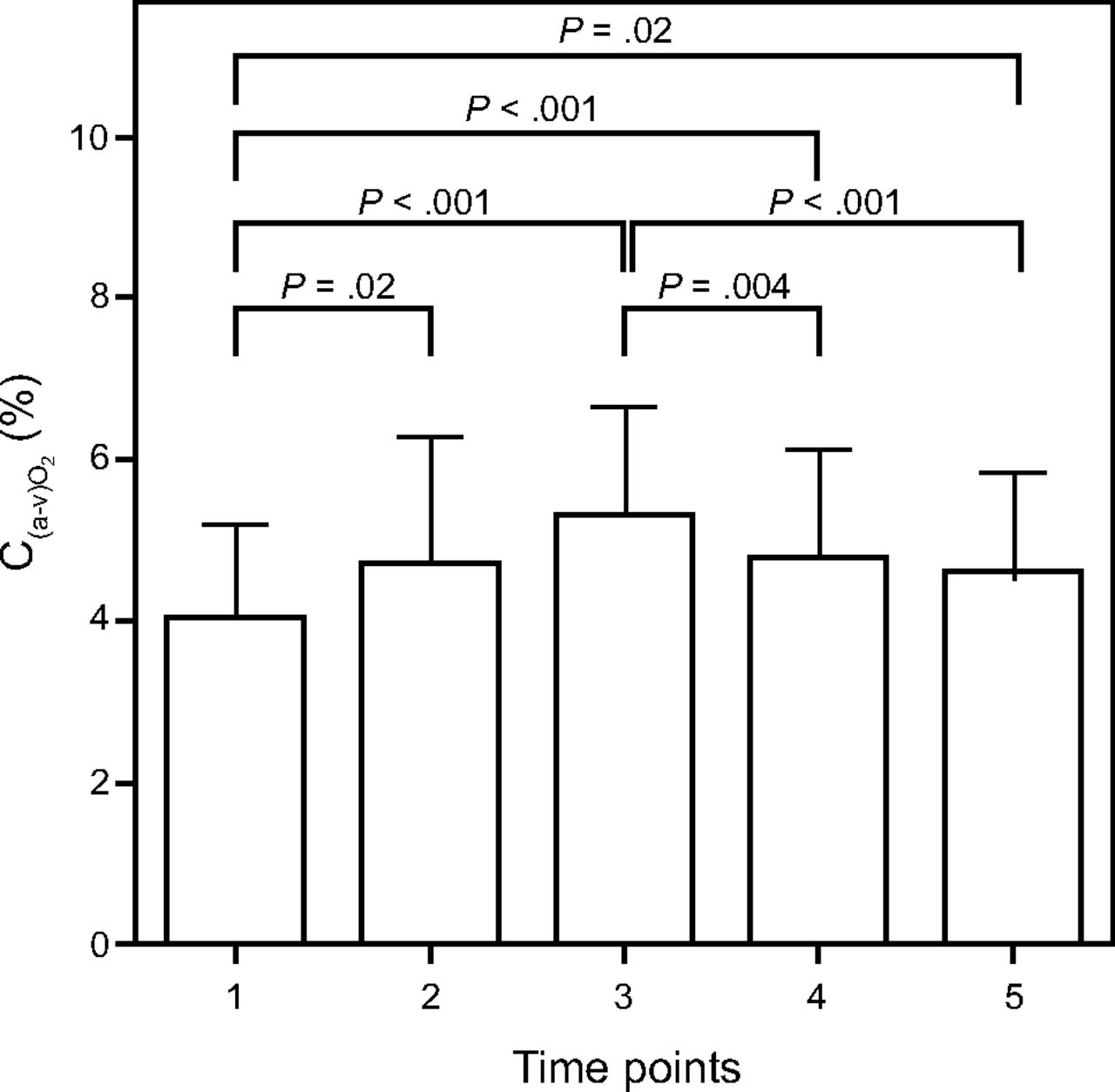
The SaO2 differences among the 5 data collection points were not significantly different (P > .02) (Fig. 2A). The arteriovenous oxygen content difference increased at ICU admission compared with intraoperative values (after anesthetic) (P = .02). During NIV application, there was a decrease in C(a-v)O2 (P < .001) when compared with extubation during spontaneous breathing (Fig. 3). Moreover, the C(a-v)O2 maintained lower values after NIV compared with the postextubation time before NIV (P < .001) (Fig. 3).

Sequential changes of the arteriovenous oxygen content difference (C(a-v)O2) in 5 time points to assess: (1) the intraoperative period (after anesthesia induction), (2) 20 min after ICU arrival (under intermittent mandatory ventilation), (3) 20 min after extubation in spontaneous breathing, (4) after 1 h of noninvasive ventilation (NIV) (immediately before NIV removal), and (5) 20 min after NIV discontinuation. Values are given as mean ± SD.
When dichotomized according to coronary artery bypass graft surgery performed on and off pump, a significant increase in blood lactate and the drop in Scv̄O2 was observed in both groups at arrival to the ICU compared with the intraoperative values (after anesthetic) (Table 2). The Scv̄O2 decreased after extubation compared with the value at admission (under invasive ventilation) in both subgroups (5.51% drop, P = .007; and 4.41% drop, P = .033, respectively) (Table 2). With respect to blood lactate, the subjects who underwent on-pump coronary artery bypass graft surgery had higher values compared with off-pump coronary artery bypass graft surgery, especially at the moment of extubation (P < .001) (Table 2).
Values of Variables Assessed in Subgroups of Subjects Who Underwent Coronary Artery Bypass Grafting On Pump and Off Pump
A significant improvement in Scv̄O2 during and 20 min after NIV was observed in both subgroups (Table 2). Blood lactate decreased during and after NIV in the on-pump subgroup (P = .01 and P = .005, respectively). However, the subjects who underwent on-pump coronary artery bypass graft surgery presented with higher blood lactate during and after NIV compared with the off-pump coronary artery bypass graft surgery (P = .02 and P = .040, respectively) (Table 2). No statistically significant differences were found in SaO2 at any moment between the groups. The C(a-v)O2 was decreased during and after NIV in the on-pump subgroup (P = .01 and P < .001, respectively) (Table 2). No differences in C(a-v)O2 were observed between the groups (Table 2).
Discussion
In the current study, the addition of NIV acutely improved tissue perfusion, as expressed by an increase in Scv̄O2 and a decrease in blood lactate in a post-coronary artery bypass graft cohort with LV dysfunction. As such, we believe that the major contribution of this study consists of demonstrating the capability of NIV to improve microvascular hemodynamic predictors in subjects undergoing coronary artery bypass graft surgery. In this context, NIV may be a valuable management approach during postoperative management to improve tissue perfusion.
Previous studies support Scv̄O2 and blood lactate as important independent predictors of morbidity and mortality after cardiac surgery.2,3,11–13 A lower (< 68%) or higher (> 80%) than normal Scv̄O2 can reflect an increased rate of oxygen extraction to match organ demand, with increased anaerobic energy production and accumulation of blood lactate.14
Our study revealed that subjects with LV dysfunction who underwent coronary artery bypass graft surgery and who were admitted to the ICU under invasive ventilation exhibited a significant decrease in Scv̄O2 after extubation during spontaneous breathing. Similar results were found by Jubran,15 who reported an important decrease in Scv̄O2 after positive-pressure removal.
There is previous evidence of positive results in subjects with heart failure after NIV application due to the capability of NIV to improve cardiac index and cardiac output.7,8,16,17 However, these studies did not evaluate tissue perfusion markers. To the best of our knowledge, this is the first study that evaluated acute NIV effects on tissue perfusion, specifically in subjects with LV dysfunction during the early postoperative period after cardiac surgery.
According to Ranucci et al,11 an Scv̄O2 cutoff of < 68% combined with a lactate value of > 3 mmol/L strongly predicted mortality. Our findings revealed that, during NIV application, an expressive lactate decrease (∼11%) occurred, while maintaining lactate at < 3 mmol/L. Moreover, the Scv̄O2 increased ∼6% compared with pre-NIV values, which suggests a potential clinical benefit in subjects with LV dysfunction during the early postoperative period after coronary artery bypass graft surgery. After NIV discontinuation, tissue perfusion improvement was maintained when compared with the moment of NIV application. In addition, tissue perfusion values were higher when compared with pre-NIV applications. Similar results were found by Chen and Ye,18 who reported a greater decrease in blood lactate with NIV application during the postoperative period of cardiac surgery. However, the aforementioned study did not report baseline cardiac function.
There is evidence that NIV could positively impact cardiac performance, possibly by reducing heart geometry.7,16,19 Positive pressure promotes an acute effect on the heart by the increase in pleural pressure, with a subsequent decrease in transmural pressure, which reduces the left-ventricle preload and afterload.20 For this reason, it has been suggested that positive-pressure application could improve myocardial contractility and cardiac performance. Khayat et al21 conducted a randomized controlled trial and found that bi-level positive airway pressure was superior to continuous positive airway pressure in improving LV ejection fraction in subjects with systolic dysfunction, which supports the use of bi-level positive airway pressure in the present study.
Based on our results, we speculated that the improvement in tissue perfusion occurred due to increases in the cardiac index and cardiac output, although these parameters were not directly evaluated in this study. Nevertheless, we provided an evaluation of C(a-v)O2, which is commonly used to reflect the capacity of organs and muscles to extract and use oxygen from the circulation. Previous studies in subjects with heart failure attribute part of the increase in C(a-v)O2 to an impairment in perfusion as a consequence of a decreased output index.22,23 In our study, we observed that, when Scv̄O2 decreased, C(a-v)O2 increased after extubation, when positive-pressure ventilation was removed. In addition, NIV application showed an increase in Scv̄O2 and a decrease in C(a-v)O2 when compared with the moment of extubation. Because no alteration was seen in arterial blood oxygenation (SaO2), it would indicate that better tissue perfusion was marked by an improvement in cardiac performance that results from better blood flow distribution.
Another plausible explanation for the improvement of tissue perfusion with NIV consists of ventilatory assistance given to the inspiratory muscles, which reduces the work of breathing. Patients with heart failure present with a blood flow deviation to the peripheral musculature during physical exertion, which leads to early dyspnea. A reduced oxidative capacity of respiratory and peripheral muscles could increase oxygen consumption with consequent mismatching of oxygen delivery and demand, even at rest. With NIV application, a drop in the work of breathing can occur, which leads to a better distribution of blood flow and, consequently, tissue perfusion.7
In the current study, when subjects were dichotomized into subgroups according to coronary artery bypass graft technique, those who underwent on-pump coronary artery bypass graft surgery had higher blood lactate during all data collection points. We observed that both coronary artery bypass graft surgery subgroups exhibited a significant decrease in blood lactate with the use of NIV. However, these results were not considered clinically relevant in the on-pump subgroup because lactate remained > 3 mmol/L despite NIV application. Cardiopulmonary bypass is often associated with a systemic inflammatory response syndrome, which promotes microcirculatory alterations and involves alterations in tissue permeability. These postoperative alterations lead to cardiac vulnerability and a decrease in tissue perfusion.11 We speculated that a longer duration of NIV application could be necessary to promote clinically relevant results in those who underwent on-pump coronary artery bypass graft surgery.
During postoperative management, Kirkeby-Garstad et al5 reported that subjects who underwent coronary artery bypass graft surgery had a markedly lower Scv̄O2 during the first and second postoperative day mobilization. However, the importance of the early onset of cardiac rehabilitation after coronary artery bypass graft surgery is well recognized. Therefore, we believe that NIV could be an additional strategy to improve the cardiopulmonary interaction, with the aim to improve tissue perfusion. In this way, NIV could be a promising tool to allow for early and safe mobilization after coronary artery bypass graft surgery. Further studies to investigate the potential value of NIV application during early mobilization in subjects after coronary artery bypass graft surgery are warranted.
The current study had limitations that must be recognized. First, Scv̄O2 and blood lactate after NIV removal were not evaluated over the long term. Second, direct serial cardiac performance measures were not obtained. Therefore, further studies are necessary to investigate how long NIV effects are maintained.
Conclusions
The acute application of NIV improved Scv̄O2 and decreased blood lactate in the subjects with LV dysfunction during the early postoperative phase after coronary artery bypass graft surgery. Thus, NIV use may improve myocardial performance, which leads to a better distribution of oxygenated blood to tissues and, therefore, better tissue perfusion.
Footnotes
- Correspondence: Solange Guizilini PhD, Department of Human Movement Sciences, Physical Therapy School - Federal University of São Paulo, Rua Silva Jardim, 136 - Edifício Central - CEP: 11015–020 Santos, Brazil. E-mail: s_guizilini{at}yahoo.com.br.
The authors have disclosed no conflicts of interest.
- Copyright © 2018 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}