

Abstract
BACKGROUND: The objective of the current study was to determine whether overnight pulse oximetry in patients with amyotrophic lateral sclerosis is prognostic of the onset of awake respiratory failure and hospital admissions.
METHODS: This was an observational study in a cohort of subjects with amyotrophic lateral sclerosis. The study included subjects with a baseline  ≥ 94% on home overnight pulse oximetry testing. Patients age ≥ 80 y and those with comorbidities and with poor short-term prognosis or sleep apnea were excluded. The subjects were classified as nocturnal desaturators according to percentage of sleep time with
≥ 94% on home overnight pulse oximetry testing. Patients age ≥ 80 y and those with comorbidities and with poor short-term prognosis or sleep apnea were excluded. The subjects were classified as nocturnal desaturators according to percentage of sleep time with  < 90% (T90) > 10%.
< 90% (T90) > 10%.
RESULTS: A total of 76 subjects were included: 40 men (53%), mean ± SD age 60 ± 14.4 y, mean ± SD body mass index 25.7 ± 4.60 kg/m2, and spinal presentation in 63.2%. After overnight pulse oximetry, 20 subjects (26%) were classified as desaturators and 56 (74%) as non-desaturators. In the first year, the subjects with nocturnal desaturation had respiratory failure more often compared with the subjects without desaturation (35% vs 10.91%; P = .02) and had a higher risk of developing respiratory failure during the course of the study (hazard ratio 2.48; P = .030). The desaturator group also had a higher rate of ≥ 1 admission (40% vs 7.3%; P = .01) and a higher likelihood of respiratory-related hospitalization (hazard ratio 2.41; P = .02). Median survival was almost 1 year less if T90 > 10% was observed in the overnight pulse oximetry: 21 months versus 32 months survival if T90 was ≤ 10%.
CONCLUSIONS: In subjects with amyotrophic lateral sclerosis, nocturnal desaturation conferred a higher risk of respiratory failure and poorer prognosis. Even in the absence of other clinical criteria, early pulse oximetry should be performed and the need for nocturnal ventilatory support assessed.
- amyotrophic lateral sclerosis
- motor neuron disease
- neuromuscular disease
- noninvasive ventilation
- overnight pulse oximetry
- respiratory failure
- survival
Introduction
Amyotrophic lateral sclerosis (ALS) is a neurodegenerative disease characterized by a progressive loss of motor neurons in the motor cortex, brain stem, and spinal cord. It has an incidence of 2–3 cases per 100,000 population and a prevalence of 6–7/100,000 population in Europe.1,2 Respiratory muscle weakness affects mortality in patients with ALS due to respiratory failure and related complications, with the initial respiratory manifestations being observed during sleep.3,4 Polysomnography and polygraphy are expensive tests with considerable waiting lists and are not available at all care levels. In this respect, home pulse oximetry is a simple technique that is valid for determining peripheral oxygen saturation ( ) during sleep.
) during sleep.
It has been postulated that, in patients with ALS, the deterioration in gas exchange during sleep may provide important information on disease prognosis. However, no studies have specifically evaluated the validity of home overnight pulse oximetry for this purpose. The aim of this study was to determine whether nocturnal desaturation could provide prognostic results related to the development of awake respiratory failure and unscheduled respiratory-related hospital admissions in a cohort of subjects with ALS.
QUICK LOOK
Current knowledge
In the course of ALS, progressive respiratory muscle weakness causes respiratory failure in the final stages of the disease. The first manifestations can be observed during sleep, and pulse oximetry is a simple technique that is valid for determining peripheral oxygen saturation. It has been postulated that alterations in gas exchange may influence the prognosis of the disease.
What This paper contributes to our knowledge
Subjects with ALS and nocturnal desaturation presented a more rapid decline to daytime respiratory failure and a higher number of hospital admissions. Analysis of these data may suggest the early use of noninvasive ventilation in patients without daytime respiratory failure but with nocturnal desaturation, even in the absence of other criteria, as well as close monitoring.
Methods
Study Design and Population
This was a retrospective cohort analysis conducted in a university hospital by using STROBE methodology for epidemiologic observational studies.5 All the subjects included in the study were from the Cordoba health-care area and were undergoing follow-up at the home mechanical ventilation unit of the Reina Sofía Hospital in Cordoba, Spain. The study was approved by the ethics and scientific research committee (CI 0729-N-18).
Subjects
Our Department of Pneumology reviewed the records of patients with ALS who were referred to us between January 2009 and June 2016. These patients fulfilled El Escorial criteria for ALS.6 The clinical data and functional tests were collected at the time of pulse oximetry. The subjects with an awake  ≥ 94% were included. The eligible population consisted of patients diagnosed in the Department of Neurology between 2009 and June 2016, according to the El Escorial criteria,6 and were referred for assessment to the home ventilation clinic. Functional tests and overnight pulse oximetry were performed; patients with an awake
≥ 94% were included. The eligible population consisted of patients diagnosed in the Department of Neurology between 2009 and June 2016, according to the El Escorial criteria,6 and were referred for assessment to the home ventilation clinic. Functional tests and overnight pulse oximetry were performed; patients with an awake  ≥ 94% with follow-up of at least 6 months were included.
≥ 94% with follow-up of at least 6 months were included.
The following patients were excluded: age ≥ 80 y; severe comorbidity (cancer, New York Heart Association class IV heart failure, chronic liver disease with the Model for End-Stage Liver Disease functional stage >12, renal failure with glomerular filtration rate < 30 mL/min); patients who at the time of performing the overnight pulse oximetry were in respiratory failure, with noninvasive ventilation (NIV), or a diagnosis of obstructive sleep apnea syndrome. The latter was determined by confirming the absence of heavy snoring, observed apneas, dry mouth and throat during sleep, nocturia or excessive daytime sleepiness (score on the Epworth scale of >12).
Clinical Variables: Data Source
Data were collected from the subjects’ clinical history and electronic medical records, which included medical information from primary and specialized care. The following anthropometric and clinical characteristics, especially those related to nocturnal hypoventilation, were collected when the home pulse oximetry was performed: orthopnea, morning headaches, non-refreshing sleep and daytime sleepiness in passive situations, form of onset (bulbar or spinal), forced spirometry while standing and in decubitus, and overnight pulse oximetry values.
Monitoring
Scheduled checkups were carried out at the home ventilation unit every 6 months in subjects without NIV, every 3 months in those with NIV, or at the subject’s request in case of clinical worsening. This study was conducted under conditions of normal medical practice, and the indication of NIV was made by following current guidelines.6,7 The outcome variables analyzed were the time (months) between performing the overnight pulse oximetry and the onset of daytime respiratory failure ( < 60 mm Hg or
< 60 mm Hg or  ≤ 90%), time (months) to the first unscheduled respiratory-related hospital admission, and survival.
≤ 90%), time (months) to the first unscheduled respiratory-related hospital admission, and survival.
Home Pulse Oximetry
Home pulse oximetry was performed by using a pulse oximeter (Pulsiox-300, Konica Minolta Sensing, Osaka, Japan). The test was explained to the subjects and their caregiver by experienced health-care staff from the sleep unit. The recording was done at home and started just before going to bed and ended on awakening; the recommended duration was a minimum of 5 h and a maximum of 7 h. The following day, the caregiver sent the pulse oximeter to the sleep unit for automatic analysis (Sofware Minolta DS5, Osaka, Japan) and manual analysis by the medical staff. The test was valid if at least 4 h of sleep had been recorded without artifacts in the  signal. The awake
signal. The awake  , mean
, mean  and percentage time recorded in pulse oximeter with
and percentage time recorded in pulse oximeter with  < 90% (T90) were analyzed.
< 90% (T90) were analyzed.
There is some controversy with regard to the definition of significant desaturation during sleep6,8; for the purposes of this study, T90 > 10% was considered clinically important. This cutoff point classified subjects as desaturators (T90 > 10%) or non-desaturators (T90 ≤ 10%). The primary objective was to compare, during the follow-up of both groups, the time (months) until the subjects presented awake respiratory failure at a checkup or, if applicable, during a hospital admission. The time to the first hospital admission and the number of admissions were also analyzed.
Statistical Analysis
A descriptive study was performed by calculating the mean ± SD for the quantitative variables, and the absolute and relative frequencies for the qualitative variables. To evaluate differences between the desaturator and non-desaturator groups, the Mann Whitney U test or the chi-square test was performed. Time to daytime respiratory failure, hospital admissions and survival were then analyzed independently by using Kaplan-Meier curves and the log-rank test. In all cases, the hazard ratio and 95% CI were calculated as an estimator of risk. All comparisons were 2-sided, and P < .05 was considered significant. Data were analyzed by using the statistical package SPSS v.25 (IBM, Armonk, New York).
Results
A total of 114 patients were referred to the home ventilation clinic, 76 of whom met the selection criteria and showed an awake  ≥ 94%; 20 subjects (26%) were classified as the nocturnal desaturation group (Fig. 1). The anthropometric and clinical characteristics of the subjects at the time that the pulse oximetry was performed are shown in Table 1. The data were similar in both groups, except for the body mass index, which was higher in the desaturator group (P = .039). From a functional point of view, there were no differences in forced spirometry values between the groups (P > .05). Spirometry in supine decubitus showed no significant differences, although the desaturator group presented a clinically relevant decrease in FVC (mean ± SD –7,7 ± 12.4% vs −14 ± 20.11%). Over the course of the study, 47 subjects (62%) started NIV, 29 (53%) in the group with T90 < 10% and 18 subjects (90%) in the group with T90 > 10% (P = .003).
≥ 94%; 20 subjects (26%) were classified as the nocturnal desaturation group (Fig. 1). The anthropometric and clinical characteristics of the subjects at the time that the pulse oximetry was performed are shown in Table 1. The data were similar in both groups, except for the body mass index, which was higher in the desaturator group (P = .039). From a functional point of view, there were no differences in forced spirometry values between the groups (P > .05). Spirometry in supine decubitus showed no significant differences, although the desaturator group presented a clinically relevant decrease in FVC (mean ± SD –7,7 ± 12.4% vs −14 ± 20.11%). Over the course of the study, 47 subjects (62%) started NIV, 29 (53%) in the group with T90 < 10% and 18 subjects (90%) in the group with T90 > 10% (P = .003).

Flow chart. OSAS = obstructive sleep apnea syndrome. T90 = percentage of recording time with  < 90%.
< 90%.
Clinical and Anthropometric Characteristics of Subjects Included in the Study
All the subjects were on ventilation in S/T mode, with a mean ± SD inspiratory positive airway pressure of 12 ± 2.8 cm H2O and mean ± SD expiratory positive airway pressure of 4.3 ± 0.6 cm H2O. The mean ± SD use ratio was 6 ± 5.05 h and the mean ± SD duration of the NIV was 14.22 ± 12.73 months. In the disease progression, only 2 subjects declined NIV, and the mean ± SD time from pulse oximetry measurement until the initiation of NIV was a little more than 27.4 ± 60 d). As shown in Table 2, with respect to the non-desaturator group, the subjects with T90 > 10% presented a higher rate of respiratory failure (55% vs 28.6%; P = .034) and more respiratory-related hospital admissions (mean ± SD 0.9 ± 0.89 vs 0.6 ± 1.21; P = .01).
Prognostic Data Observed in the Study Groups
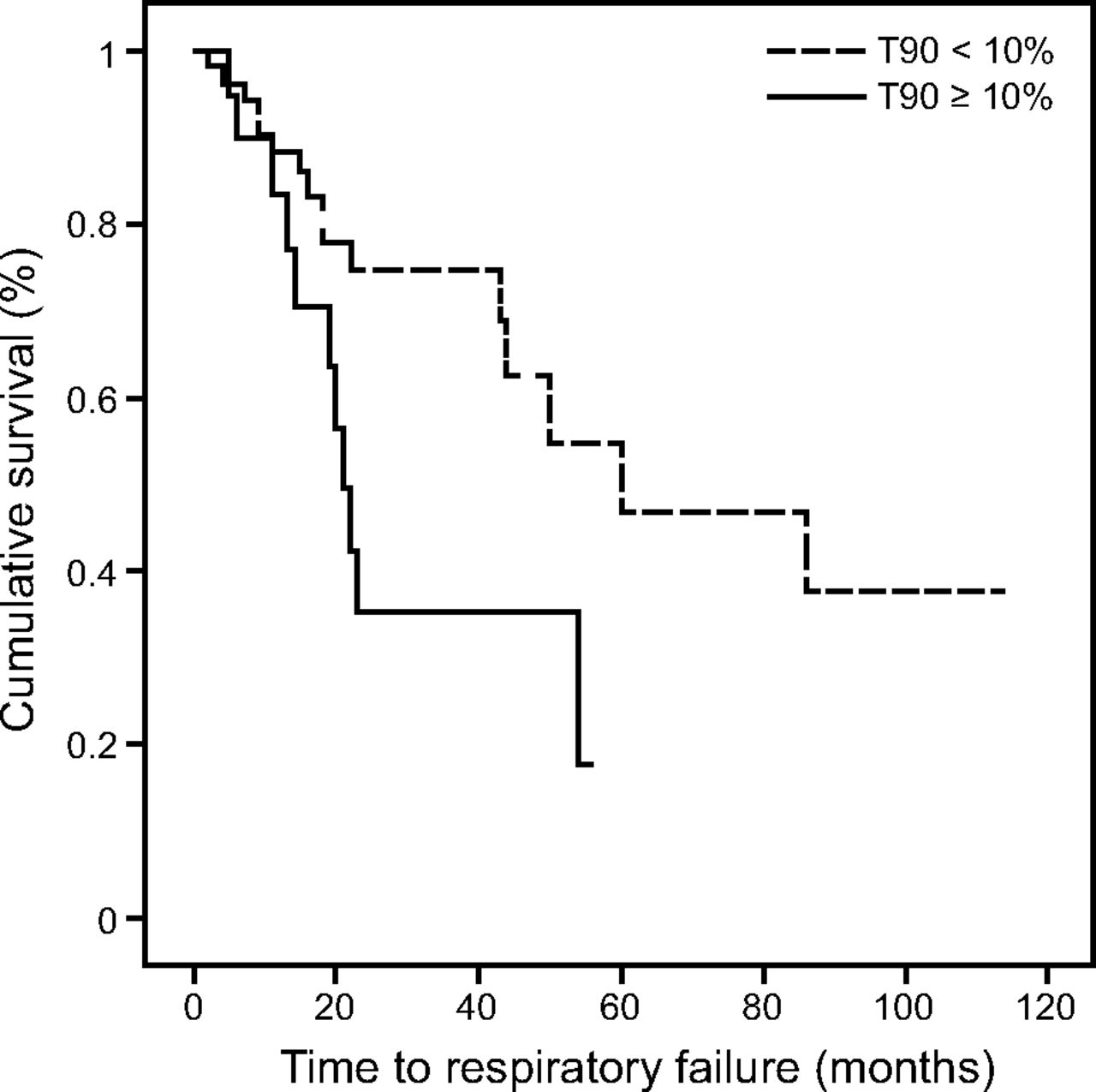
During the first year, 35% of the subjects with nocturnal desaturation developed respiratory failure compared with 11% in the non-desaturator group. When the curves of both groups were compared according to respiratory failure (Fig. 2), statistically significant differences were obtained (P = .02), which showed a median of 21 (range, 14–54) months compared with 60 (range, 22–92) months observed in the subjects without nocturnal desaturation. Furthermore, during the study, the subjects with T90 > 10% had a higher risk of developing respiratory failure (hazard ratio 2.479, 95% CI 1.12–5.47; P = .030).

A Kaplan-Meier curve for respiratory failure according to degree of nocturnal desaturation.
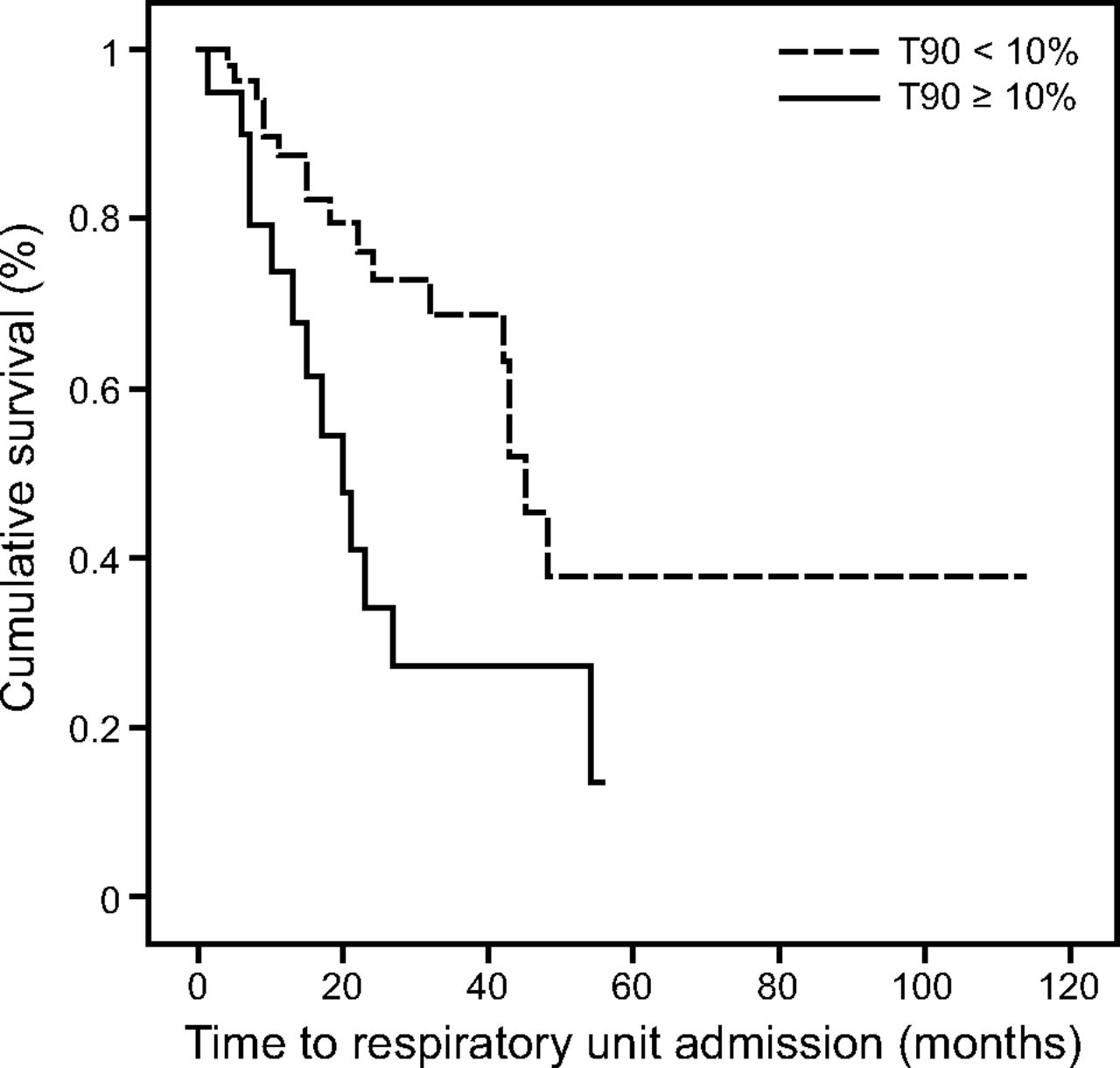
In the first year, 40% of the subjects with nocturnal desaturation had at least one hospital admission compared with 7.27% in the non-desaturator group; differences were also observed when the curves were compared (P = .01) (Fig. 3). Similarly, the nocturnal desaturation group presented a higher likelihood of respiratory-related hospital admissions (hazard ratio 2.411, 95% CI 1.17–4.98; P = .01). When the survival curves stratified by desaturator or non-desaturator (Fig. 4) were compared, no statistically significant differences were found (P = .17), although a tendency toward longer survival was observed in the group without nocturnal desaturation, with a median survival of 32 (range, 15–67) months versus 21 (range, 12–40) months observed in the nocturnal desaturation group.

A Kaplan-Meier curve for respiratory-related admission stratified by degree of nocturnal desaturation.
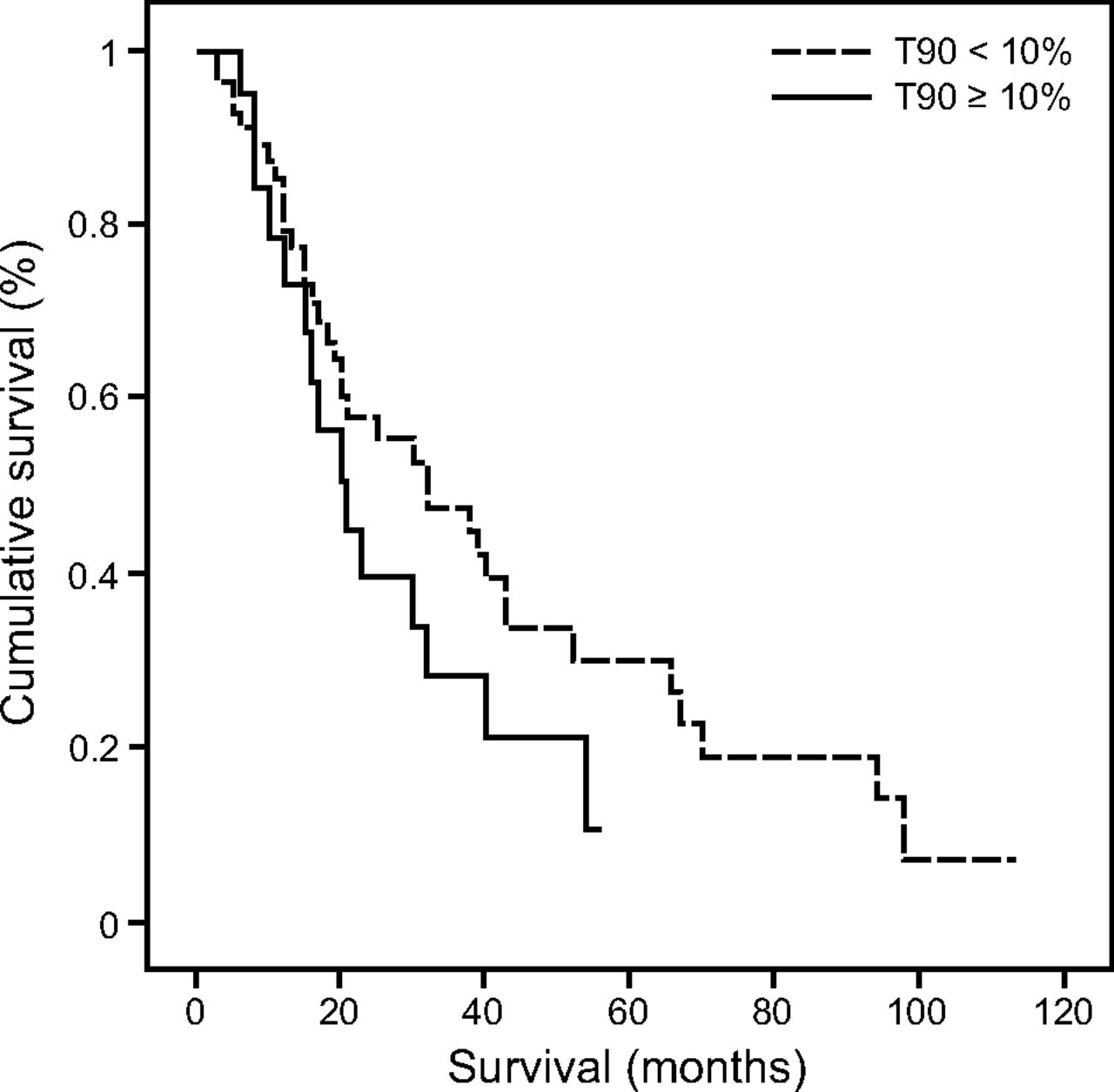
Kaplan-Meier survival curve according to the degree of nocturnal desaturation.
Discussion
Evaluation of the role of overnight pulse oximetry in 76 subjects with ALS showed that those with desaturation during sleep presented a more rapid respiratory decline to daytime respiratory failure and a higher number of hospital admissions. In ALS, some factors have been associated with poorer evolution, including bulbar involvement.9-11 However, in our study, this presentation was not related to greater nocturnal desaturation, a finding also observed by other researchers.12 The measure of bulbar dysfunction in ALS is complex as well as are the factors associated with a poor prognosis.11,13 It is probable that the poor prognosis of bulbar ALS is related to alterations in swallowing (malnutrition) and repetitive microaspirations (tracheobronchitis and aspiration pneumonia).
In a study conducted to evaluate the relationship between FVC < 50% and nocturnal  , no significant difference in
, no significant difference in  values were observed among the subjects with FVC > 50% or < 50% of predicted.14 In our research, baseline FVC was also similar in both groups, although the percentage decline in FVC in decubitus was twice as high in the desaturator group, probably due to diaphragmatic weakness.15,16 As in our study, nocturnal desaturation predicted more rapid deterioration of gas exchange and progression to respiratory failure. According to these researchers, many patients are symptomatic at higher FVCs and manifest evidence of nocturnal hypoxemia.14
values were observed among the subjects with FVC > 50% or < 50% of predicted.14 In our research, baseline FVC was also similar in both groups, although the percentage decline in FVC in decubitus was twice as high in the desaturator group, probably due to diaphragmatic weakness.15,16 As in our study, nocturnal desaturation predicted more rapid deterioration of gas exchange and progression to respiratory failure. According to these researchers, many patients are symptomatic at higher FVCs and manifest evidence of nocturnal hypoxemia.14
To our knowledge, there are no studies that specifically measured home overnight  to determine prognostic factors. The results described are generally obtained from polysomnography or polygraphy studies.7 In a study of 131 subjects with ALS and in whom polygraphy was performed, it was observed that 35% of the subjects showed nocturnal desaturation, defined as
to determine prognostic factors. The results described are generally obtained from polysomnography or polygraphy studies.7 In a study of 131 subjects with ALS and in whom polygraphy was performed, it was observed that 35% of the subjects showed nocturnal desaturation, defined as  < 90% for 5 min, with a minimum value of 85% or a T90 of 30% of sleep.10 However, a T90 of 30% is a very restrictive criterion.
< 90% for 5 min, with a minimum value of 85% or a T90 of 30% of sleep.10 However, a T90 of 30% is a very restrictive criterion.
In our study, it should be underlined that 26% of the subjects had nocturnal desaturation in their baseline pulse oximetry; this is unusual if  > 94% is observed during wakefulness.17 Nevertheless, this finding is important because, in our cohort, a little more than one third of the subjects (35%) with nocturnal desaturation developed respiratory failure during the first year, and, during the course of the study, the subjects with nocturnal desaturation had a 71% higher likelihood of presenting nocturnal desaturation compared with the subjects without nocturnal desaturation. Moreover, the time to respiratory failure was 21 months versus 60 months in the subjects with no desaturation. It, therefore, is important to initiate NIV as soon as possible, even in the absence of other clinical or functional criteria because respiratory failure is one of the main causes of morbidity and mortality in patients with ALS.18
> 94% is observed during wakefulness.17 Nevertheless, this finding is important because, in our cohort, a little more than one third of the subjects (35%) with nocturnal desaturation developed respiratory failure during the first year, and, during the course of the study, the subjects with nocturnal desaturation had a 71% higher likelihood of presenting nocturnal desaturation compared with the subjects without nocturnal desaturation. Moreover, the time to respiratory failure was 21 months versus 60 months in the subjects with no desaturation. It, therefore, is important to initiate NIV as soon as possible, even in the absence of other clinical or functional criteria because respiratory failure is one of the main causes of morbidity and mortality in patients with ALS.18
With regard to urgent hospitalization, in a retrospective study of 262 subjects, the first admission for respiratory failure had a negative effect on survival.19 In our cohort, the subjects with nocturnal desaturation presented with a shorter time to first urgent admission to a respiratory medicine unit, of 20 months versus 45 months, in the subjects who did not desaturate, and a higher risk of respiratory-related hospital admission; both factors determine poorer survival.18-20 These results support the need to perform overnight pulse oximetry that will prompt the clinician to carry out an early evaluation of other risk factors. At present, the indication for NIV according to nocturnal desaturation is still variable.6-8
Nevertheless, until new evidence becomes available, the results of our study support the finding that, even in the subjects who are minimally symptomatic, a T90 > 10% was associated with a poor prognosis. We, therefore, recommend that this result is taken into account when initiating NIV, one of the great advances in the management of ALS that has helped to improve the quality of life and survival of patients.9,21,22 In our study, the onset of NIV was delayed an average of 27 d after the pulse oximetry was performed; this time should probably be shortened, but, in addition to nocturnal pulse oximetry, other criteria (clinical and spirometric) are used to initiate NIV.6-8,23
Respiratory failure, together with the clinical and functional assessment of the patient, are factors that determine the indication for NIV.7,24,25 This was established in our study, which might explain the higher percentage of subjects with NIV in the desaturator group. This could minimize the negative effect of early respiratory failure on mortality. In this regard, it should be underlined that survival in the subjects with nocturnal desaturation was almost 1 year shorter with respect to the subjects with no desaturation. However, this was probably not statistically significant, as previously mentioned, due to the beneficial effect of NIV.9,21,22 Moreover, ALS is a heterogeneous disease, with a great number of factors that influence prognosis.22
Some limitations should be taken into account. First, the study was retrospective, although the sources of information from the electronic records were reliable and provided sufficient information to generate the results and conclusions of our study. The diagnosis of bulbar ALS was made in the Department of Neurology by a change in speech, swallowing, and salivation. However, the ALS functional rating scale was not always available, so it was not always possible to establish a correlation with nocturnal  at the time of pulse oximetry. Furthermore, the subjects were recruited from a single health-care area, which may be a limitation. However, this offered an additional advantage in that clinical care was similar and the same clinical practice guideline recommendations were followed.6,7
at the time of pulse oximetry. Furthermore, the subjects were recruited from a single health-care area, which may be a limitation. However, this offered an additional advantage in that clinical care was similar and the same clinical practice guideline recommendations were followed.6,7
Conclusions
In the subjects with ALS, nocturnal desaturation was associated with more rapid progression to respiratory failure in the first year as well as a shorter time to first urgent admission and a higher number of hospitalizations. The results of our study showed that, in subjects who did not present daytime respiratory failure, nocturnal desaturation (in the absence of other criteria) is essential to guide the initiation of NIV and to prevent a more rapid respiratory decline, with a poorer prognosis.
Footnotes
- Correspondence: Pilar Font Ugalde MD, Medicine Department, Av Menendez Pidal, 7, 14004, Córdoba, Spain. E-mail: fougp{at}hotmail.com
The authors have disclosed no conflicts of interest.
- Copyright © 2020 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}