

Abstract
BACKGROUND: Manual rib cage compression is a chest physiotherapy technique routinely used in clinical practice. However, scientific evidence remains scarce on the effects of manual rib cage compression on airway clearance and oxygenation in mechanically ventilated patients.
METHODS: Anesthetized pigs were intubated via the trachea and mechanically ventilated. To create atelectasis, artificial mucus was infused into the airway. Each pig was randomly assigned to 1 of 2 groups: closed suctioning alone (control group, 7 pigs), or manual rib cage compression combined with closed suctioning (manual rib cage compression group, 8 pigs). Hard and brief rib cage compression synchronized with early expiratory phase was tested. Mucus clearance and oxygenation were assessed after the intervention. Sequential changes of hemodynamics were assessed after the intervention.
RESULTS: During hard manual rib cage compression, the mean ± SD peak expiratory flow increased to 44 ± 7 L/min compared with 31 ± 7 L/min without treatment (P < .001). Manual rib cage compression combined with endotracheal suctioning increased mucus clearance compared with closed suctioning alone (mucus amounts, 5.5 [3.4–9.4] g vs 0.7 [0.5–2.0] g; P = .004); however, it did not improve gas exchange and radiologic findings. There were no significant differences in hemodynamic variables between the 2 groups.
CONCLUSIONS: Our findings indicated that hard and brief manual rib cage compression combined with closed suctioning was safe and led to improvement of mucus clearance; however, no effectiveness was confirmed with regard to oxygenation and ventilation.
Introduction
Retention of airway secretions can result in serious clinical complications in patients on mechanical ventilation.1-4 Mucus retention narrows or occludes airways,5,6 causes breathing discomfort, and leads to atelectasis and gas exchange impairment.7 In the acute care setting, mucus retention is related to significantly higher mortality and morbidity.8 Manual rib cage compression (MRCC) is a chest physiotherapy technique routinely used in clinical practice.9-11 However, scientific evidence on the effects of MRCC on airway clearance and oxygenation in mechanically ventilated patients remains unclear because of the variety of techniques.
A previous animal study showed that a hard and brief MRCC technique applied during the early expiratory phase increases expiratory flow and mucus movement compared with a soft and gradual MRCC technique applied during the late expiratory phase.12 Nevertheless, it is not clear whether MRCC combined with endotracheal suctioning promotes mucus clearance and improves oxygenation in patients with mucus retention. The objective of this study was to determine whether a combination of hard MRCC and endotracheal suctioning could improve mucus clearance and oxygenation in well-controlled mechanically ventilated pigs with retention of artificial mucus.
QUICK LOOK
Current knowledge
Mechanically ventilated patients often have impaired airway mucus clearance. Manual rib cage compression is routinely used in clinical practice. However, the effect of manual rib cage compression on airway clearance and oxygenation in these patients remains unclear.
What this paper contributes to our knowledge
In this prospective randomized animal study, manual rib cage compression combined with closed suctioning resulted in a larger amount of mucus clearance than did closed suctioning alone but did not improve gas exchange.
Methods
Animal Preparation
This study was conducted at the University of Tsukuba, Japan. The protocol was approved by the institution’s animal research committee. Animals were managed according to the National Institute of Health guidelines for the Use and Care of Animals. Fifteen female pigs (mean ± SD, 33 ± 2 kg) were anesthetized by using midazolam and ketamine, and were restrained in a supine position. Intravenous lines were installed at the ear vein of each pig, and a continuous infusion of pentobarbital was delivered. Tracheostomy was performed with the pig under local anesthesia by using 1.0% lidocaine solution and a 7-mm inner-diameter endotracheal tube (ETT) placed in the trachea. The animals were then ventilated with LTV-1000 ventilators (CareFusion, San Diego, California).
To instill artificial mucus into the airways, a closed suctioning catheter system (Trachcare, Ballard Medical Products, Draper, Utah) was connected to the ETT. Mechanical ventilation was set as follows: pressure control,  1.0, PEEP 10 cm H2O, peak inspiratory pressure 20 cm H2O achieved tidal volume of 6–8 mL/kg, and breathing frequency was adjusted to maintain normocapnia. Internal ETT cuff pressure was maintained at 25 cm H2O. The pigs were paralyzed with a loading (0.6 mg/kg) and maintenance (0.4-0.6 mg/kg/h) dose of vecuronium. Femoral artery catheter was surgically inserted to monitor the systemic arterial pressure and to collect blood samples. A pulmonary artery catheter (Model 744F8, Edwards Lifesciences, Irvine, California) was also placed via femoral vein to measure hemodynamic variables, including stroke volume and cardiac output.
1.0, PEEP 10 cm H2O, peak inspiratory pressure 20 cm H2O achieved tidal volume of 6–8 mL/kg, and breathing frequency was adjusted to maintain normocapnia. Internal ETT cuff pressure was maintained at 25 cm H2O. The pigs were paralyzed with a loading (0.6 mg/kg) and maintenance (0.4-0.6 mg/kg/h) dose of vecuronium. Femoral artery catheter was surgically inserted to monitor the systemic arterial pressure and to collect blood samples. A pulmonary artery catheter (Model 744F8, Edwards Lifesciences, Irvine, California) was also placed via femoral vein to measure hemodynamic variables, including stroke volume and cardiac output.
Model of Atelectasis
To create atelectasis, artificial mucus was infused into the airways by using the closed suction method. The technical details are shown in our previous experimental reports.13,14 Briefly, the artificial mucus was made by mixing 1.6% polyethylene oxide powder and 0.1% methylene blue in a phosphate buffered saline solution, and, to prepare thinner artificial mucus, iopamidol was mixed with the artificial mucus at a ratio of 3:2.13,14 Dynamic viscoelasticity of the solution was measured with a controlled shear rate rheometer, at a driving frequency of a 1 rad/s. The loss modulus (G′′) of the artificial mucus was 1.6 Pa, and the storage modulus (G′) was 0.97 Pa. The artificial mucus infusion was continued at a rate of 4 mL/min for 10 min (total of 48 g) with reference to a previous animal study.15 After the mucus infusion, the closed suction catheter was changed to the other catheter. The animals were maintained on mechanical ventilation for 30 min after administration of the mucus.
Hard-Type Rib Cage Compression
A single operator, a trained nurse (HH), performed the hard MRCC. The nurse applied short (∼1 s) and strong bilateral compressions.12 Hand pressure pads were used to assess the force of each compression.14 In preliminary experiments, we confirmed that hand pressure reflects esophageal pressure. Compressions were synchronized with the start of the expiratory phase.
Endotracheal Suctioning
An experienced nurse (YY) performed the endotracheal suctioning according to the guidelines of the American Association for Respiratory Care.16 Neither hyperventilation nor manual hyperinflation was performed before or after endotracheal suctioning. Closed suction was performed by using the closed suctioning catheter (12 French) system mentioned above. A premeasured catheter was inserted, without applying suction, to the ETT tip. When in place, suction was applied at a pressure of –150 mm Hg for 15 s while simultaneously withdrawing the catheter. The weight of the suctioned mucus was calculated by subtracting the weight of the container before suction from its weight after suction.
Data Collection
Heart rate and mean arterial pressure were monitored by using a Philips IntelliVue MP50 Patient Monitor (Philips Medizin Systeme, Böblingen, Germany). Cardiac output was monitored by using Vigilance II (Edwards Lifesciences). Arterial blood gases were measured by using blood drawn from the femoral artery via an ABL 735 blood gas analyzer (Radiometer Copenhagen, Copenhagen, Denmark). Ex-piratory tidal volume, airway pressure, and airway flow were recorded by using a CP-100 pulmonary monitor (Bicore, Irvine, California). Radiologic images were taken by using a C-arm (DHF-105CX, Hitachi, Japan). Radiologic findings were assessed from the atelectasis score (0, clear lung fields; 1, plate-like atelectasis or slight infiltration; 2, partial atelectasis; 3, lobar atelectasis; and 4, bilateral lobar atelectasis)17 and 0–10 cm visual analog scale by 2 investigators blinded to all experimental information.
Study Design
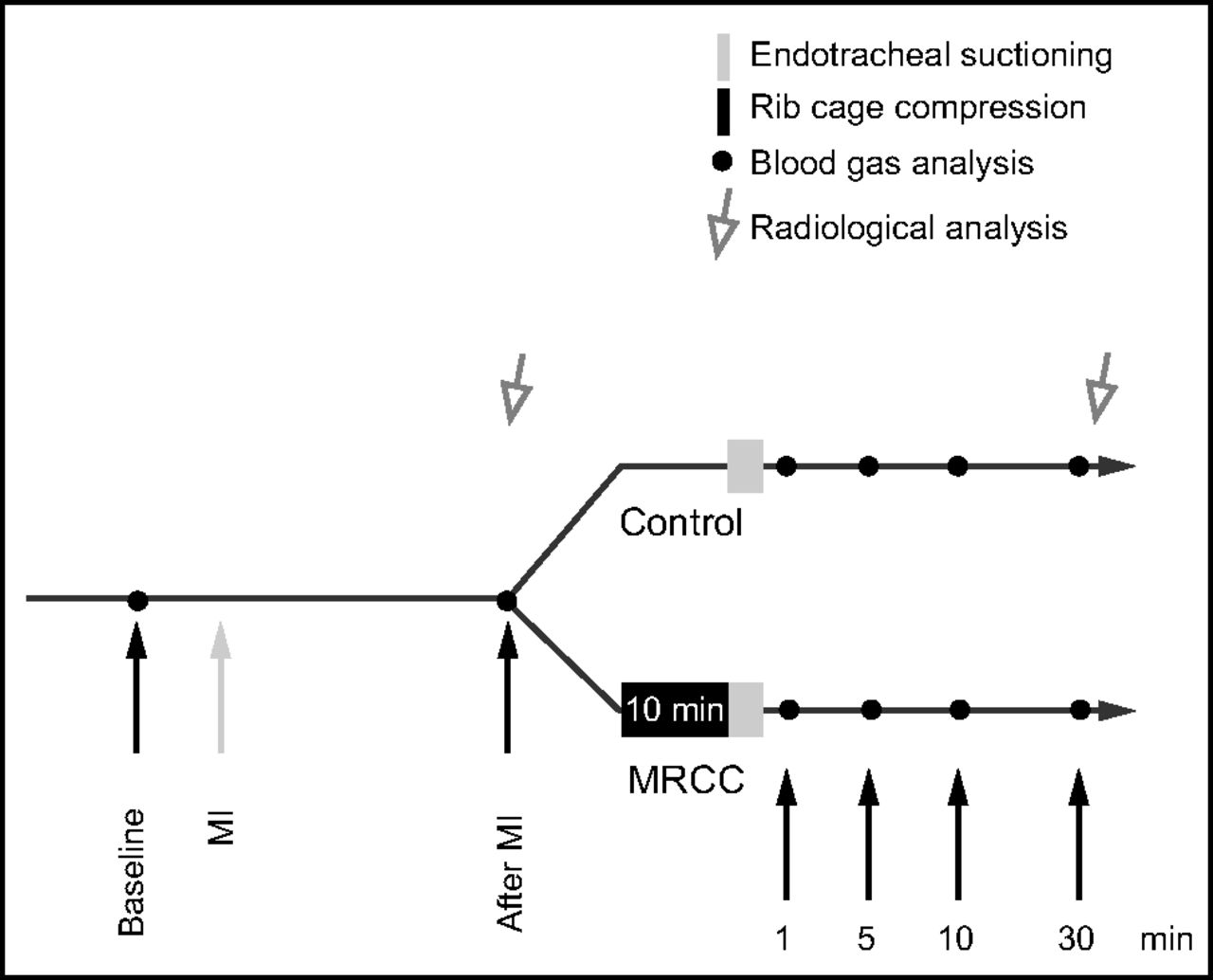
The experimental protocol is illustrated in Figure 1. After the first radiologic images were taken, the pigs were randomly assigned to 2 groups: closed suctioning alone (control group, 7 pigs), or hard MRCC combined with closed suctioning (MRCC group, 8 pigs). After the experiments, the pigs were sacrificed with an intravenous injection of 10 mL (10 mEq/10 mL) potassium chloride solution.

Experimental protocol. A researcher applied a 10-min session of manual rib cage compression (MRCC). Radiologic images were taken at baseline (before randomization) and the end of the period. MI = mucus infusion.
Statistical Analysis
All values are reported as a mean ± SD unless otherwise specified. Parametric and nonparametric analyses were used in accordance with the results of the Shapiro-Wilk test. Paired t test or the Wilcoxon rank-sum test were used to compare before and after treatment measurements. Intra-intergroup differences were compared by using one-way analysis of variance with adjusted Bonferroni correction. Repeated measures analysis of variance was used to determine intragroup differences. Specific intergroup differences and time points of these differences were determined by using the Bonferroni correction for multiple comparisons. All tests were performed as 2-sided, with a significance level of 5%. All analyses were performed by using SPSS version 25 software (SPSS, Chicago, Illinois).
Results
Baseline characteristics of the animals in the study groups are shown in Table 1. There were no differences in body weight, hemodynamic variables, and gas exchange parameters before the artificial mucus infusion. During the compression, the mean ± SD peak expiratory flow (PEF) increased to 44 ± 7 L/min compared with 31 ± 7 L/min without treatment (P < .001). The mean ± SD expiratory tidal volume increased to 345 ± 46 mL compared with 215 ± 87 mL (P < .001) without treatment. As shown in Figure 2, MRCC combined with endotracheal suctioning increased mucus clearance compared with closed suctioning without MRCC (P = .004). The median range values of mucus amounts (g) in the control and MRCC groups were 0.7 (0.5-2.0) g and 5.5 (3.4-9.4) g, respectively.
Baseline Characteristics (before mucus infusion)

Sputum volume produced after control and manual rib cage compression (MRCC) interventions. Horizontal lines denote median value, upper and lower edges represent the 25th and 75th percentiles, and whiskers represent the 10th and 90th percentiles. * P < .01, compared with control.
The results of  /
/ and
and  are shown in Figure 3. With regard to oxygenation, there were no significance differences in
are shown in Figure 3. With regard to oxygenation, there were no significance differences in  /
/ before mucus infusion or at baseline. After mucus infusion,
before mucus infusion or at baseline. After mucus infusion,  /
/ decreased in all the pigs. Throughout the experiment, there were no significance differences in
decreased in all the pigs. Throughout the experiment, there were no significance differences in  /
/ between the control and MRCC groups (Fig. 3A). With regard to ventilation,
between the control and MRCC groups (Fig. 3A). With regard to ventilation,  for both groups increased significantly compared with the baseline after the mucus infusion. There were no significance differences in
for both groups increased significantly compared with the baseline after the mucus infusion. There were no significance differences in  between the control and MRCC groups throughout the experiment (Fig. 3B).
between the control and MRCC groups throughout the experiment (Fig. 3B).

Changes in (A)  /
/ (P/F) and (B)
(P/F) and (B)  in the study groups. There were no significance differences between the 2 groups. Data are shown as means with 95% confidence intervals. MRCC = manual rib cage compression; MI = mucus infusion.
in the study groups. There were no significance differences between the 2 groups. Data are shown as means with 95% confidence intervals. MRCC = manual rib cage compression; MI = mucus infusion.
Radiologic data are expressed as median (interquartile range). There were no significance differences between the groups in the atelectasis scores before and after the interventions (Fig. 4A). There were also no significance differences between the groups in visual analog scale scores before and after the interventions (Fig. 4B). The effects of MRCC on hemodynamics are shown in Table 2. There were no significance differences in heart rate, mean arterial pressure, and cardiac output between the groups.

Changes in (A) atelectasis scores and (B) visual analog scale (VAS) scores in the study groups. Horizontal lines denote median value, the upper and lower edges represent the 25th and 75th percentiles, and whiskers represent the 10th and 90th percentiles. There were no significance differences between the 2 groups.
Sequential Changes in Variables of Hemodynamics
Discussion
The purpose of the present study was to investigate whether the combination of MRCC and following closed suctioning could improve mucus clearance and oxygenation under well-controlled experimental settings. The present study demonstrated that MRCC increased the PEF and improved mucus clearance; however, the maneuver did not improve oxygenation or radiologic findings. An animal study by Marti et al12 compared 2 different MRCC techniques and investigated their respective effects. The soft and gradual MRCC technique did not increase PEF; however, hard and brief MRCC significantly increased PEF and mucus movement.12 MRCC generates an expiratory flow bias that is believed to move secretions toward the central airways through a 2-phase gas-liquid transport.18,19 A previous study showed that mucus clearance significantly improves by increasing PEF to 40–60 L/min.20
The findings of the present study were that MRCC increased PEF, and, via the 2-phase gas-liquid transport mechanism, increased mucus clearance. Nevertheless, similar to previous findings,9 we did not find any positive effect on gas exchanges and radiologic findings. Contrary to our findings, a randomized crossover study found that a combination of MRCC and manual hyperinflation improved mucus clearance and oxygenation in subjects on mechanical ventilation.10 Manual hyperinflation, which involves lung ventilation by using a manual resuscitation bag, is a technique used in patients on mechanical ventilation to assist airway reopening.21 The reopening maneuver was not applied in our study, and MRCC alone could not remove the peripheral secretions nor re-expand the collapsed area. Therefore, a larger amount of mucus clearance might not lead to improved oxygenation.
Although not significantly different between the groups, our results showed that MRCC exacerbated  and
and  . A possible cause of this phenomenon is a decrease in end-expiratory lung volume. Furthermore, MRCC may exacerbate alveolar collapse (because of the compressive effect), which leads to decreasing the ventilation-perfusion ratio. In our study, all the pigs received mechanical ventilation with PEEP of 10 cm H2O, and the protective effects of PEEP gradually stabilized the collapsed area; thus,
. A possible cause of this phenomenon is a decrease in end-expiratory lung volume. Furthermore, MRCC may exacerbate alveolar collapse (because of the compressive effect), which leads to decreasing the ventilation-perfusion ratio. In our study, all the pigs received mechanical ventilation with PEEP of 10 cm H2O, and the protective effects of PEEP gradually stabilized the collapsed area; thus,  increased in the MRCC group at the 30-min point. Another possible explanation is that an insufficient amount of mucus was removed from the airway due to the limitations of the suction protocol in our study. Increasing PEF contributes to moving mucus from the periphery to the proximal airways. Mucus retained in the proximal airway may influence ventilation and resistance parameters. Further studies are necessary to assess longer time courses or improved suctioning protocol to remove airway mucus completely.
increased in the MRCC group at the 30-min point. Another possible explanation is that an insufficient amount of mucus was removed from the airway due to the limitations of the suction protocol in our study. Increasing PEF contributes to moving mucus from the periphery to the proximal airways. Mucus retained in the proximal airway may influence ventilation and resistance parameters. Further studies are necessary to assess longer time courses or improved suctioning protocol to remove airway mucus completely.
We found no changes in hemodynamic parameters, in agreement with a previous study.12 In general, vigorous physical stimuli such as MRCC can cause sympathetic activation and result in tachycardia and hypertension in conscious patients. In the present study, however, the animals were anesthetized by using midazolam and ketamine, followed by a continuous infusion of pentobarbital and a muscle relaxant, vecuronium. Hence, it is likely that the pigs could hardly perceive physical stimulation associated with MRCC. Randomized trials have found that the heart rate was slightly but significantly reduced compared with controls in the postmaneuver measurement.22,23 MRCC imposes external pressure on the rib cage and may change venous return. Nevertheless, the repercussion of the maneuver on the main hemodynamic variables was low. In addition, it is important to note that more significant hemodynamic changes may also occur in patients with hemodynamic instability.
Limitations
There were a few limitations of this study to consider. First, to assess the effects of MRCC on expiratory flow and avoid potential biases due to the animals’ spontaneous exhalation, the pigs were paralyzed by using neuromuscular blockade. Thus, our findings are not entirely applicable to patients with spontaneous breathing. However, recent clinical studies investigated the effects of MRCC in specific conditions such as those that require a neuromuscular blockade24 or mucus hypersecretion.25 Our experiment may contribute qualitative principles to consider the effectiveness of the intervention in specific conditions. Second, we were unable to assess atelectasis by using computed tomography due to a lack of equipment. Instead, we assessed atelectasis with visual analog scale scores from 0 to 10 cm by marking a single line on a scale anchored by the terms blackness and whiteness. Thus, the diagnosis of atelectasis may have lacked optimal sensitivity. Third, our study did not apply manual or ventilator hyperinflation; further research is needed to assess the effect of combining hyperinflation and MRCC. Fourth, our study demonstrated the safety of the intervention in terms of hemodynamic parameter; however, in elderly individuals who are debilitated or frail, we need to take into consideration the possibility of rib injury. Fifth, although pigs are commonly used to study airway mucus clearance, there seems to be considerable differences in morphology and function, such as collateral ventilation, among different species.26 Therefore, translational clinical studies require further corroboration in humans.
Conclusions
Our findings indicated that hard MRCC combined with closed suctioning was safe and led to improvement of mucus clearance; however, no effectiveness was confirmed with regard to oxygenation and ventilation. Further well-conducted clinical studies are needed to thoroughly investigate the effects of MRCC.
ACKNOWLEDGMENTS
We thank Thomas Mayers, Medical English Communications Center, University of Tsukuba, for grammatical revision of this paper.
Footnotes
- Correspondence: Yoshiaki Inoue MD PhD, Department of Emergency and Critical Care Medicine, Faculty of Medicine, University of Tsukuba, Tsukuba, Ibaraki, 305-8575 Japan. E-mail: yinoue{at}md.tsukuba.ac.jp
This work was performed at the University of Tsukuba.
This work was supported in part by a Grant-in-Aid for Young Scientists B from the Ministry of Education, Culture, Sports, Science and Technology of Japan (16K20746) and the Japan Society for the Promotion of Science.
The authors have disclosed no conflicts of interest.
- Copyright © 2020 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}