

Abstract
BACKGROUND: Oxygen therapy provided via high-flow nasal cannula (HFNC) improves gas exchange lung compliance and results in increased lung expiratory volumes. Previous data indicate that hyperbaric and humid states improve the olfactory thresholds compared to hypobaric and dry conditions. This prospective, observational study aimed to determine the impact of oxygen delivery through HFNC on olfactory function in subjects admitted to the ICU for acute respiratory failure (ARF).
METHODS: 30 subjects who were admitted to the ICU for ARF underwent an olfactory sniff test before and after oxygen therapy with HFNC. Baseline olfactory function of subjects with ARF was also compared against 30 healthy controls. Odor threshold (OT), odor discrimination (OD), odor identification (OI) and global olfactory score (TDI) were recorded for all subjects.
RESULTS: The OT, OD, OI, and TDI scores were significantly higher in the control group compared to the baseline scores of the subjects with ARF (P < .001 for all comparisons). In subjects with ARF, administration of oxygen with HFNC led to significant improvements in OT (P = .02), OD (P = .001), OI (P = .02), and TDI (25.5 ± 3.8 vs 27.1 ± 3.5, P < .001) scores.
CONCLUSIONS: Our results indicate that subjects with ARF had relative olfactory dysfunction compared to healthy controls. These results also suggest that implementation of HFNC to relieve hypoxemia in subjects presenting with ARF can lead to a significant improvement in olfactory function.
- acute respiratory failure
- oxygen therapy
- high-flow nasal cannula
- Sniffin’ sticks test
- olfactory function
Introduction
Acute respiratory failure (ARF) is an immediate clinical presentation that may occur as a consequence of abnormalities in the central nervous system, neuromuscular system, upper and lower airways, lung parenchyma, and the cardiovascular system.1 Oxygen therapy is the cornerstone of treatment, which may be delivered via several routes, including mask, nasal cannula, CPAP, or high-flow nasal cannula (HFNC).2 Nasal cannula, face masks, and bag-valve masks are usually utilized in the management of ARF in the emergency setting. However, high pressure, low temperature, and low humidity of the air administered through these devices leads to dryness of the nose, mouth, and throat, which is closely related to patient discomfort.
In contrast to standard oxygen therapy via a nasal cannula, which can supply  = 1.0 at a maximum of 15 L/min, HFNC is capable of delivering up to 60 L/min of heated, humidified gas via nasal prongs.3 Recent trials have reported that HFNC has noninferior clinical efficacy compared to conventional low-flow oxygen-supplementation devices.4,5 Heated and humidified air provided via HFNC improves gas transfer and may increase end-expiratory lung volume.6 Moreover, implementation of HFNC enables the reduction of
= 1.0 at a maximum of 15 L/min, HFNC is capable of delivering up to 60 L/min of heated, humidified gas via nasal prongs.3 Recent trials have reported that HFNC has noninferior clinical efficacy compared to conventional low-flow oxygen-supplementation devices.4,5 Heated and humidified air provided via HFNC improves gas transfer and may increase end-expiratory lung volume.6 Moreover, implementation of HFNC enables the reduction of  by washing nasopharyngeal dead space with high-flow air and therefore facilitates resolution of the existing hypoxia.7-11
by washing nasopharyngeal dead space with high-flow air and therefore facilitates resolution of the existing hypoxia.7-11
Smelling is one of the 5 major sensory abilities in humans. Olfaction is initiated by the binding of odor molecules to the olfactory receptors located in the peripheral olfactory neurons. The signal is then transmitted through the olfactory nerve to the olfactory bulb and ultimately to the olfactory cortex, allowing for multiple signals to be processed to form a synthesized olfactory perception.12 In addition to several neurological and psychiatric diseases that might influence olfaction, environmental conditions have also been shown to affect olfactory perception.13-16 Previous data revealed that hyperbaric and humid states improve olfactory thresholds compared to hypobaric and dry conditions.17 This prospective, observational study aimed to determine the impact of oxygen delivery through a HFNC on olfactory function in subjects admitted to the ICU for ARF.
Quick Look
Current knowledge
Smelling is one of the 5 major sensory abilities in humans and might be influenced by the presence of acute respiratory failure and by the mode of oxygen given during treatment. High-flow nasal cannula (HFNC) has been used increasingly as a bridge between low-flow oxygen therapies and CPAP to reduce the need for CPAP or intubation. However, the flow generated by HFNC may impair olfactory function.
What this paper contributes to our knowledge
Subjects with acute respiratory failure had relative olfactory dysfunction compared to healthy controls. Implementation of oxygen therapy via HFNC not only relieved hypoxemia but also led to significant improvement in olfactory function, probably due to the warm and humid flow provided.
Methods
Subject Selection
This prospective study was conducted on subjects admitted to the ICUs of Sancaktepe Training and Research Hospital and Süreyyapasa Training and Research Hospital between November 2018 and December 2018. Informed consent was obtained from all individuals included in the study. This study was approved by the Institutional Ethical Committee and the study was performed in accordance with the recent version of the Helsinki Declaration (KAEK-033/01.11.2018). The following were the inclusion criteria: admission to ICU for oxygen support (eg, COPD exacerbation, asthma, hypertensive pulmonary edema, and postoperative atelectasis), Glasgow coma scale score of 15, spontaneous respiration, breathing frequency of > 20–24 breaths/min,  < 90%, and hemodynamic stability. Exclusion criteria were upper respiratory tract infection within the previous 2 weeks, prior head trauma, neurodegenerative diseases, major depression, active malignancy, and structural nasal pathology (eg, nasal polyps, allergic rhinitis, subjects with nasogastric feeding tube, and septal deviation). To eliminate any confounders that might influence olfactory tests, patients using medications that might affect odor perception and patients > 65 y of age were not included in this study. Power calculations based on our pilot study with 20 subjects revealed that at least 21 subjects were required to study the impact of HFNC on olfactory function (pre-HFNC global olfactory score of 24.6 ± 5.1 mm vs post-HFNC global olfactory score of 28.3 ± 4.8 mm, effect size 0.75, alpha error 0.5, power 0.95).18 The study included 30 subjects admitted to the ICU with hypoxia and 30 age- and sex-matched healthy volunteers as the control group.
< 90%, and hemodynamic stability. Exclusion criteria were upper respiratory tract infection within the previous 2 weeks, prior head trauma, neurodegenerative diseases, major depression, active malignancy, and structural nasal pathology (eg, nasal polyps, allergic rhinitis, subjects with nasogastric feeding tube, and septal deviation). To eliminate any confounders that might influence olfactory tests, patients using medications that might affect odor perception and patients > 65 y of age were not included in this study. Power calculations based on our pilot study with 20 subjects revealed that at least 21 subjects were required to study the impact of HFNC on olfactory function (pre-HFNC global olfactory score of 24.6 ± 5.1 mm vs post-HFNC global olfactory score of 28.3 ± 4.8 mm, effect size 0.75, alpha error 0.5, power 0.95).18 The study included 30 subjects admitted to the ICU with hypoxia and 30 age- and sex-matched healthy volunteers as the control group.
HFNC Intervention
HFNC therapy was initiated with a flow of 40 L/min,  0.40, and 34°C. All subjects received routine hemodynamic and arterial blood gas monitoring. After 48 h from admission, subjects were reevaluated for the further need for HFNC or discontinuation of HFNC (ie, improved clinical findings and laboratory values, normalized breathing frequency, decreased secretions, and near-normal arterial blood gases) and the smell test was repeated.
0.40, and 34°C. All subjects received routine hemodynamic and arterial blood gas monitoring. After 48 h from admission, subjects were reevaluated for the further need for HFNC or discontinuation of HFNC (ie, improved clinical findings and laboratory values, normalized breathing frequency, decreased secretions, and near-normal arterial blood gases) and the smell test was repeated.
Olfactory Testing
The Sniffin’ Stick test (Heinrich Burghart, Wedel, Germany), consisting of three subtests that measure odor threshold (OT), odor discrimination (OD) and odor identification (OI), was used to evaluate olfactory function in subjects receiving HFNC and in controls. Odorants were presented in felt-tip pens, the tips of which were impregnated with 4 mL odorant fluid or odorant substance dissolved in propylene glycol. Each pen was presented only once, for 3 s, held approximately 2 cm from the edge of the nostril, without touching the subject’s skin.
A single-staircase technique was used to determine the OT for n-butanol with a forced choice of 3 options. Three pens from 16 triplets of pens were presented in a randomized order, with 2 pens containing the solvent and the third the odorant. Presentation of the triplets to a subject occurred every 20 s. Two correct identifications of the pen containing the odor or 1 incorrect identification triggered a reversal of the staircase to the next higher or the next lower dilution step, respectively. Threshold was defined as the mean of the last 4 of 7 staircase reversals and was scored between 1 and 16.
Sixteen triplets of pens were presented for OD, with 2 pens containing the same odorant and 1 pen containing the target odorant. Subjects were blindfolded with a sleeping mask to prevent visual detection of the target pen. The subjects were allowed to sniff the odor once and were asked to identify the sample that had a different smell. The interval between each individual pen was 3 s, and the presentation of triplets was separated by 20 s. The OD subtest score ranged between 0 and 16.
Sixteen common odors were used for OI. Using a forced multiple-choice paradigm, identification of individual odors was performed from a list of 4 verbal descriptors each. There was an interval of 20 s between odor presentations. The OI subtest score ranges between 0 and 16.
Finally, scores of the 3 subtests were added to obtain the global olfactory score (TDI). Subjects with a score > 30 were defined as normosmic; those with a score between 16 and 30 were defined as hyposmic, and subjects with a score < 16 were defined as anosmic.19 The testing took 20–25 min for each subject, and supplemental oxygen therapy was paused only during the sniffing.  and
and  were monitored during olfactory testing and the test was paused if oxygen saturation decreased below 80%.
were monitored during olfactory testing and the test was paused if oxygen saturation decreased below 80%.
All subjects underwent a baseline olfactory testing 30 min before the HFNC therapy. The OT, OD, OI, and TDI values from controls were compared with that of the HFNC subjects at baseline. To compare the baseline and post-treatment OT, OD, OI, and TDI values, olfactory testing was repeated at 48 h after HFNC treatment was started. The primary outcome of the study was the change in TDI score from baseline to post-HFNC in subjects receiving HFNC due to ARF.
Statistical Analysis
Statistical analyses were performed with SPSS 20 for Windows (IBM, Armonk, New York). Continuous variables were presents as means ± SD, and the categorical variables were presented as numbers and percentages. The Shapiro-Wilk test was used to determine whether the variables were distributed normally. Continuous variables were compared with Student t test and the Mann-Whitney U test. Comparison of the categorical variables was performed with the chi-square test. Paired sample test was used to pre- and post-HFNC olfactory test scores. A P value < .05 was considered statistically significant.
Results
The study was conducted on 60 subjects (mean age 64.3 ± 9.3 y) and included 20 female subjects (33.3%) and 40 male subjects (66.7%). There was no significant difference in age (65.4 ± 11.2 y vs 63.2 ± 6.9 y, P = .35) or gender (20 male subjects and 10 female subjects in each group, P > .99) between groups.
The OT, OD, OI, and TDI scores were significantly higher in the control group compared to the baseline scores of the subjects with ARF (P < .001 for all comparisons, Table 1). Subjects with ARF received oxygen supplementation through an HFNC for a mean of 54 ± 13 h. A significant improvement was noted both in  (81.3 ± 4.1% vs 90.4 ± 4.5%, P < .001) and
(81.3 ± 4.1% vs 90.4 ± 4.5%, P < .001) and  (57.2 ± 3.6 mm Hg vs 77.9 ± 8.2 mm Hg, P < .001) 24 h after HFNC. In subjects with ARF, administration of oxygen with HFNC led to significant improvements in OT (4.9 ± 1.6 vs 5.4 ± 1.6, P = .02), OD (9.7 ± 1.8 vs 10.4 ± 1.5, P = .001), OI (10.9 ± 1.6 vs 11.2 ± 1.5, P = .02), and TDI (25.5 ± 3.8 vs 27.1 ± 3.5, P < .001) scores (Table 2, Fig. 1).
(57.2 ± 3.6 mm Hg vs 77.9 ± 8.2 mm Hg, P < .001) 24 h after HFNC. In subjects with ARF, administration of oxygen with HFNC led to significant improvements in OT (4.9 ± 1.6 vs 5.4 ± 1.6, P = .02), OD (9.7 ± 1.8 vs 10.4 ± 1.5, P = .001), OI (10.9 ± 1.6 vs 11.2 ± 1.5, P = .02), and TDI (25.5 ± 3.8 vs 27.1 ± 3.5, P < .001) scores (Table 2, Fig. 1).
Comparison of Age, Gender and Pre-HFNC Olfactory Test Results
Olfactory Test Results Before and After HFNC in Subjects With Acute Respiratory Failure
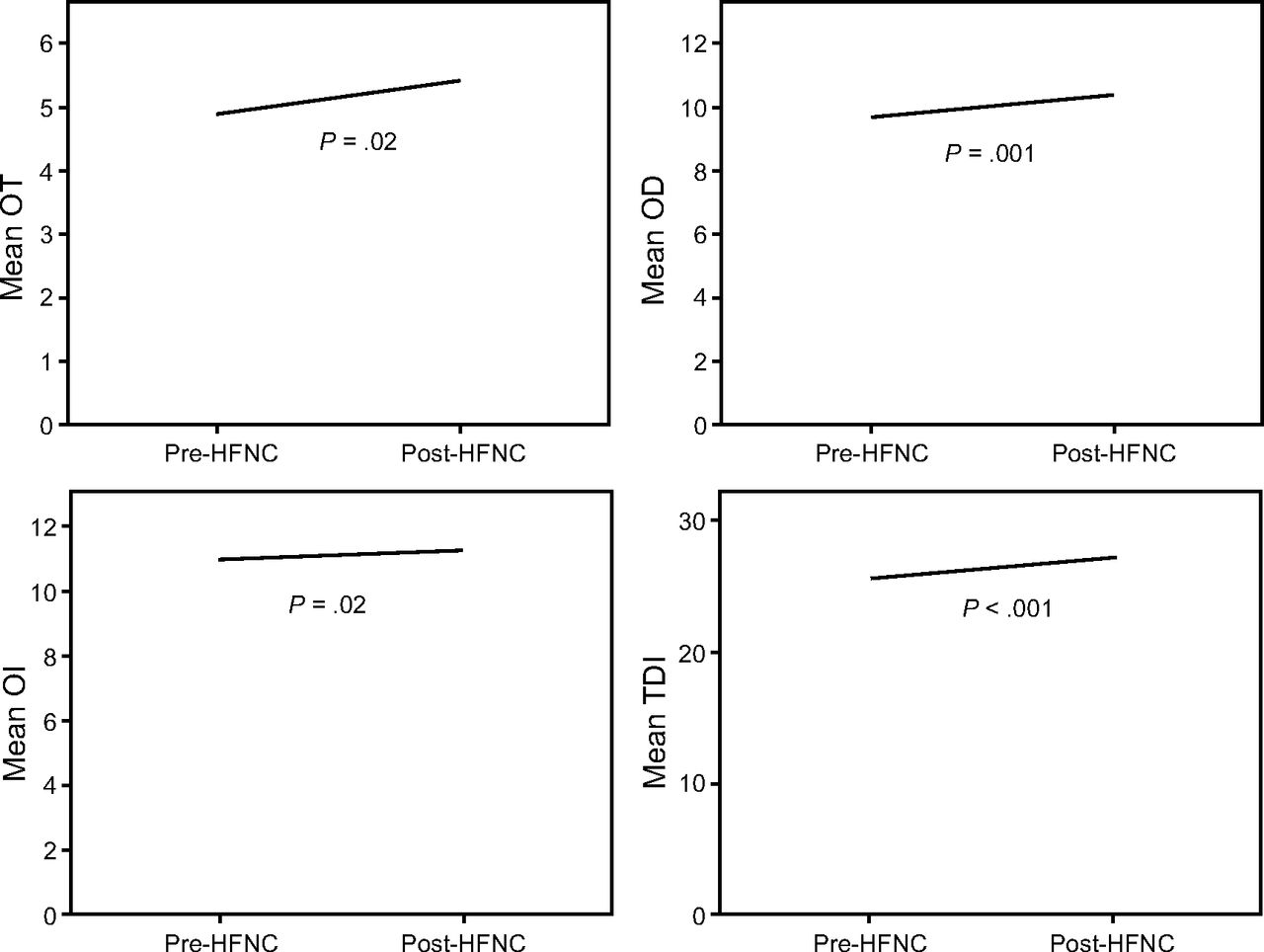
Change in odor threshold (OT), odor discrimination (OD), odor identification (OI), and global olfactory score (TDI) after implementation of high-flow nasal cannula (HFNC) in subjects with acute respiratory failure.
Discussion
This study was performed to investigate the impact of oxygen delivery via HFNC on olfactory function in subjects with ARF. Our results indicate that HFNC leads to significant improvement in OT, OD, OI, and TDI, which are valid and reliable measures of olfactory function. As shown in the comparison of baseline olfactory test results of subjects receiving HFNC and controls, OT, OD, OI, and TDI are impaired in subjects with ARF compared to healthy controls.
Oxygen therapy might be administered via several routes, including nasal cannula, face masks, or nasal prongs, which are considered traditional oxygen therapy.20 In traditional oxygen therapy, the maximum flow is 15 L/min, and room air is added to enhance flow, although this results in decreased oxygen concentration.21,22 Moreover, high flow across the nasal cannula causes patient discomfort as a consequence of the dryness of the nose, mouth, and throat in patients with ARF when it is given with inadequate humidity and temperature.23,24 In contrast to oxygen therapy with nasal cannula, HFNC rapidly relieves symptoms and enhances oxygenation by reducing oxygen dilution and inspiratory nasopharyngeal resistance and creating a moderate positive airway pressure effect that is associated with alveolar recruitment and thus with an increase in end-inspiratory lung volume.25 Beyond the mentioned physiological advantages, HFNC also ensures patient comfort as a result of the increased temperature and humidity of the oxygen obtained with this device.
Our findings indicate that implementation of HFNC in patients with ARF improves smell perception, as demonstrated with the results of the Sniffin’ Stick test. There are 4 major factors affecting the concentration of smell in the air: temperature, atmospheric pressure, humidity, and air flow. Vapor pressure increases by elevating heat and humidity, resulting in enhanced smell diffusion and facilitated smell identification.26 It has already been reported that increased temperature and humidity enhance the circulation capacity of odor molecules.17 When physiological functioning of the respiratory tract is considered, the nasopharyngeal region heats inspiratory air to 37°C and converts the air inspired to 100% relative humidity, which requires heat energy.27,28 However, in the case of high-flow, the nasal region is exposed to dry, cold air and may become dry and irritated because the relative humidity does not reach 100%. We believe that avoidance of local irritation and improved diffusion of odor molecules obtained with HFNC is the leading mechanism of the improvement in smell perception observed in our study group.
Dewan et al29 assessed olfactory function before and after treatment with via nasal cannula in subjects with COPD who required prolonged periods of oxygen therapy, but the authors found no significant difference. It has been reported that prolonged oxygen therapy via nasal cannula leads to local irritation, inflammation, and dryness in the nasal mucosa.30,31 Nasal mucosa has an important role in smell function; therefore, we suppose that a lack of recovery in smell perception despite resolution of hypoxia may be due to the local irritation of nasal mucosa caused by prior exposure to dry, cold air in patients using nasal cannula.
One of the main findings of our study was the relative olfactory dysfunction observed in subjects with ARF, most probably due to the local and generalized effects of hypoxemia, as well as mouth breathing, which is usually encountered in patients with acute hypoxemia and hampers the transmission of odor molecules from the nose to the olfactory mucosa.32 Moreover, mucus viscosity is increased by extravasations in the airway due to hypoxia, resulting in a challenge in the binding of odor molecules to the olfactory receptors.33,34 In addition to local effects, hypoxemia significantly decreases the activity of brain regions such as the thalamus, prefrontal cortex, posterior parietal cortex, and hippocampus, which are responsible for processing smell perception.35,36 Finally, as reported in previous research, hypoxia causes a significant decline in cognitive function that particularly affects OD and OI.37 To our knowledge, our study is the first to demonstrate the beneficial effects of oxygen therapy via HFNC on olfactory function in subjects admitted to the ICU for ARF. Olfactory dysfunction impairs quality of life in several ways: nutritional deficits associated with decreased appetite and enjoyment of eating, lack of maintaining personal hygiene, and greater depressive symptoms and loneliness.38 Any olfactory dysfunction should therefore be taken seriously to prevent the occurrence of these hazardous complications of olfactory loss. Clinicians should pay attention to usage of HFNC, particularly in patients at high risk for olfactory dysfunction, to maintain health-related quality of life.
Our study has some limitations. The physiological advantages of HFNC were not investigated in this study. Olfactory testing was performed 48 h after treatment with HFNC was started. Delayed testing over a longer period may provide additional information concerning the long-term effects of HFNC on smell perception. In addition, patient comfort, which is expected to be favorable with the use of HFNC compared to traditional oxygen therapy via nasal cannula, was not been studied. However, with the huge body of evidence regarding the benefits of implementation of HFNC instead of nasal cannula, a direct comparison of these 2 methods might create ethical issues. Finally, all subjects with ARF received oxygen therapy of 6 L/min through a face mask for a mean of 3.2 ± 0.8 h before HFNC was started; this could have influenced pre-HFNC olfactory test results.
Conclusions
Our findings indicate that subjects with ARF have relative olfactory dysfunction compared to healthy controls. Our results also indicate that implementation of HFNC to relieve hypoxemia in subjects presenting with ARF can lead to a significant improvement in olfactory function. Larger studies are needed in select patient groups using various pressure levels and durations.
Footnotes
- Correspondence: Esra Adiyeke MD, Department of Anesthesiology and Reanimation, University of Health Sciences, Sancaktepe Education and Research Hospital, Emek Mahallesi, Namık Kemal Cad. No. 54, 34785 Sancaktepe, Istanbul, Turkey. E-mail: esasaladiyeke{at}gmail.com
The authors have disclosed no conflicts of interest.
- Copyright © 2020 by Daedalus Enterprises





{kind=link}