

Abstract
BACKGROUND: Respiratory therapists (RTs) play important roles in providing ventilator support to patients in hospitals. They are on the front line in respiratory cases and work with physicians to help patients survive. However, questions remain regarding whether the mental health conditions at work are protected and secured for RTs. This study aimed to explore the risk factors of mental illness for RTs and to design an app to allow individual RTs to seek assistance at an earlier stage.
METHODS: A total of 642 RTs from 107 two-tiered hospitals in Taiwan were randomly selected to complete a 44-item, 5-category questionnaire regarding emotional labor and mental health in 2019. Exploratory factor analysis, the Rasch model, descriptive statistics, the nonparametric Mann-Whitney U test, the Kruskal-Wallis test for unpaired t test, and one-way analysis of variance were performed to examine the demographic characteristics and emotional labor and mental health factors that influence RTs' mental health. An app was then designed to evaluate their mental health status.
RESULTS: A total of 352 questionnaires were eligible, with a return rate of 54.8% (352 of 642). About 62.8% came from medical centers and 37.2% from regional hospitals. There were 311 (88.4%) women and 41 (11.6%) men, with a mean ± SD age of 37 ± 9.5 y. Six construct factors were extracted from the responses. The overall reliability of the emotional labor and mental health questionnaire for each subscale beyond 0.70 was evident based on internal consistency and stability in the data. Four risk factors (ie, basic emotional expression, superficial emotional control, emotional diversity extent, and weekly work hours) influenced RT mental health. All findings were applied to design an app for RTs to evaluate their mental health at work.
CONCLUSIONS: Four risk factors were verified to influence RT mental health. An app was developed to detect their mental health and allow them to seek assistance at an earlier stage.
Introduction
Respiratory therapists (RTs) play important roles in providing ventilatory support to patients in ICUs and hospital emergency departments. RTs are not only trained in cardiopulmonary care, but they also specialize in the care and therapeutic work of people with pulmonary diseases. They are on the front line in hospitals and provide respiratory care and work with physicians to help in patient survival.
Two decades ago, RTs in Taiwan encountered several challenges and changes, including the introduction of the RT Act in 2001, which defined RTs as independent professionals who are part of the essential workforce ensuring medical quality in critical care. Until 2013, Taiwanese law1 stipulated the fundamental role of RTs in hospitals and ensured that these roles are performed in health care settings.2
In recent years, RTs have also played a vital role in the quality of care of elders3 and patients experiencing problems associated with increasing levels of air pollution in an industrial society. RTs are the only health care clinicians who continuously receive education and training regarding mechanical ventilation. As a result, ventilators are one of the many health care services provided by RTs to help patients. RTs provide constant monitoring and assessment to patients by modifying ventilator settings as a patient's condition improves or worsens during a treatment regimen. As such, RT-related health care units are frequently found in the ICU and the emergency department. In Taiwan, respiratory care is clinically new but has become indispensable over the past decade.4
To obtain the knowledge and skills required for respiratory care in a health care setting, RTs need regular training courses in line with their daily clinical tasks and work load,4 such as junior and senior roles of health care.5 Furthermore, they are responsible for cost containment and accountability in hospitals.6,7
Emotional labor is the process of managing feelings and expressions to fulfill the emotional requirements of a job. Regarding mental health in the workplace, emotional labor is often encountered by front-line medical staff because administrators expect high quality-of-care services from them to meet the organization's goals. RTs and other front-line workers are expected to coordinate, control, or even suppress their emotions regarding the demands of clients, patients, or administrators at work.8,9
A conflict between workers' rights and duty is a prevalent concern.10 These include focusing on organization-oriented emotion over staff emotion,11 hoping that staff focus their efforts properly to satisfy the needs of the organization and clients more than their own needs and then manage (or properly adjust) their work-related emotions at a higher priority.12
It is difficult to define emotional labor.13,14 Workers should be trained and allowed to practice properly adjusting their emotions without suppressing their internal emotions. Failing to adjust to one's ability to deal with the conflict of work rights and duty carries a substantial burden of long-term emotional labor. Inevitably, this mental health burden will lead to stagnation of work performance.15 Conversely, workers who possess positive emotions can create a healthy environment and can maintain the quality of care as well as client satisfaction, whereas negative emotions can increase the worker's burnout and decrease job satisfaction.16,17 In this study, we aimed to evaluate the mental health of RTs.
At the Trade Review Conference in 2018, Taiwan was designated by the World Trade Organization as a well-developed country and is among the highest ranked nations in terms of mental-health spending. Numerous organizations and institutions have launched a series of mental health promotion programs.18 Emotional labor was found to result in emotional exhaustion, negative emotion, burnout at work,19,20 and mental health issues, thus directly causing stress, burnout, and low productivity.21–24
Lee et al8 disclosed that 4 mental domains, namely basic emotional expression, superficial emotional control, interaction extent, emotional diversity (ie, emodiversity) extent, and deep emotion camouflage, correlated highly and positively with mental health issues at work. The capability to deal with the conflict of work rights and duty is urgently needed by workers, particularly to overcome moderate emotional exhaustion, depersonalization, and low personal accomplishment at work.25,26 Cheung et al27 used latent profile transition analysis to examine whether emotional labor has changed over time and how to balance lifestyle without conflict of interest at workplace. However, there have been no studies on the risk factors associated with the mental health issues of RTs to date.
Surveys on labor-related emotions for nurses in Taiwan medical centers28 and Taiwan Catholic hospitals8 lacked information about the mental health of RTs, which motivated us to conduct this study. We aimed to evaluate the risk factors of mental health problems resulting from the emotional labor subscales and the demographic characteristics of RTs in Taiwan, and to design an app to help individual RTs understand their own mental health status, allowing them to seek mental health consultation at an earlier stage.
Quick Look
Current Knowledge
Emotional labor is the process of managing feelings and expressions to fulfill the emotional requirements of a job. Emotional labor is often encountered by front-line medical staff. Failure to adjust the conflict of work rights and duty carries a substantial burden of long-term emotional labor. This mental health burden could lead to stagnation of work performance.
What This Paper Contributes to Our Knowledge
Four risk factors were found to influence the mental health of respiratory therapists at work: basic emotional expression, superficial emotional control, emotional diversity, and weekly work hours.
Methods
Subjects
All RTs from 107 2-tiered hospitals in Taiwan (ie, 82 regional hospitals and 25 medical centers) were targeted to respond to a 44-item questionnaire. According to the statistics from the Taiwan Society for Respiratory Therapy, 1,521 RTs (753 from regional hospitals and 768 from medical centers) were registered in January 2019. Accordingly, if the CI was set at 0.05 ± 5% and applied to the population of 1,521 registered RTs, a minimum of 318 respondents were required to reach an adequate sample size. We estimated the percentage of candidate's refusal to respond at 40%; therefore, the minimum number of subjects was 530 [n = 318/(1 – 0.4)].
We delivered 6 copies of the 44-item questionnaire to the 107 targeted hospitals. A total of 642 (ie, 6 × 107) RTs with at least 3 months of experience working in a hospital were randomly selected and invited to complete the emotional labor and mental health survey in March 2019. This study was approved by the Institutional Review Board of Show Chwan Memorial Hospital (approval ID 1080105) before data collection. All hospital and subject identifiers were stripped.
Considerations of RTs rights, interest, privacy, and an informed consent form were taken into account when sending the mail to each hospital along with the 44-item questionnaire. The recipients were allowed to decline and not answer the questionnaire. Respondents were asked to mail the questionnaire to our study clerk in an envelope we provided for that purpose after completion.
Emotional Labor and Mental Health Questionnaire
The 44-item questionnaire was composed of 2 major parts (ie, emotional labor and mental health), in addition to questions about demographic characteristics. The 24-item emotional labor questionnaire contained those items regarding proper interaction attitudes toward patients designated by the organizations, including 7 items regarding basic emotional expression, 3 items on superficial emotional control, 3 items on interaction extent, 4 items regarding emodiversity extent, and 7 items on deep emotion camouflage.9,11,13,14 The contents of these 5 subscales are described below; see the representative items in Table 1 or the link in Reference 29 for detailed information. All of the emotional labor and mental health questions were rated from 1 to 5 (ie, from strongly agree to strongly disagree). Higher scores denote a more severe mental health problem.
Reliability Analysis and Rasch Analysis
Basic emotional expression is the degree to which the respondent expressed genuine heartfelt emotions toward the patient or client during their interaction. Superficial emotional control is the degree to which the respondent reported having hidden emotions from a patient or client during their interaction. Interaction extent includes actively raising questions, discovering health care issues, and participating in the team decisions on patient diagnosis and treatment. Emodiversity extent is the degree to which the respondents expressed emotions that they did not actually feel but were appropriate to express at that time. Deep emotion camouflage involves facing irrationality in a friendly manner, facing your fears, and seeing things from the patient's standpoint.
The second part of the emotional labor and mental health questionnaire was the 20-item mental health scale, which was derived from the World Health Organization self-reporting questionnaire in line with no emotional/mental disease symptoms and with stable and harmonious emotion/mentality as a whole.
Exploratory Factor Analysis of the Questionnaire
An exploratory factor analysis was performed to determine the number of factors retained in the data. The criterion of factor loadings was set at 0.50. Furthermore, as suggested by Fornell and Larcker,30 we used the validity significance (eg, average variance explained > 0.5) and t values on component reliability (> 0.60) at a significant level.
Rasch Analysis
When ordinal responses from RTs on questions were not congruent with the requirement of equal interval nature for further statistical analysis, we performed Rasch analysis31 using the Winsteps software32 to transform the ordinal responses into interval logit (ie, log odds) scores,33 which are suitable for regression analysis to extract the key factors influencing mental health issues among RTs. Furthermore, we examined the construct fitting to the Rasch model's expectation using the criteria of mean square errors in infit and outfit statistics, within an acceptable range of 0.5–1.5 in comparison to the classic test theory with factor loadings in exploratory factor analysis.34
Development of a Mental Health Analysis App for of RTs
A mobile app was designed by the authors for individual RTs to examine their mental health status, allowing them to seek appropriate consultations and treatments at an earlier stage.
Data Analysis
SPSS 18.0 for Windows (IBM, Armonk, New York) and MedCalc 9.5.0 for Windows (MedCalc, Ostend, Belgium) were used to perform descriptive statistics, exploratory factor analysis, nonparametric Mann-Whitney U test, Kruskal-Wallis test for unpaired t test, and one-way analysis of variance to examine the demographic characteristics influencing the scores of the RTs' emotional labor and mental health. A box plot was drawn to display the distribution of subscales in comparison. Multiple regression analysis was performed to determine the key factors influencing the mental health of RTs. A significant level of type 1 error was set at 0.05.
Results
Demographic Statistics
A total of 352 questionnaires were eligible, for a return rate of 54.8% (352 of 642, greater than the minimum number of subjects determined at the beginning of the study). The demographic data of the RTs are shown in the online supplement (see the supplementary materials at http://www.rcjournal.com). Approximately 62.8% of responses came from medical centers and 37.2% from regional hospitals. There were 311 (88.4%) women and 41 (11.6%) men, with a mean ± SD age of 37 ± 9.5 y. The frequencies of participants' educational levels were as follows: college (ie, 2-y degree), 17 (4.8%); university (ie, 4-y degree), 294 (83.5%); and graduate school, 41 (11.6%).
The number of unmarried (single or divorced) respondents accounted for 61.3% of the responses, while that of married subjects accounted for 38.6%. Only the categories of age, marital status, and RT ability presented significant statistical differences in frequency distribution at the hierarchical level. Other detailed information about the sample is provided in the online supplement (see the supplementary materials at http://www.rcjournal.com).
Construct Factors Extracted from the Study Data
Five construct factors comprising 19 items were extracted from the emotion labor questionnaires, and 13 items formed the mental health scale. All 32 items had factor loadings (ie, an equivalent correlation to the specific factor or domain) > 0.6 (see Table 1). The overall reliabilities beyond 0.70 for each subscale were evident based on internal consistency and stability in data.
The t values across all domains were significant (Table 1). All reliabilities of domains were above 0.60, and all average variances were explained. However, one of the superficial emotional control scores with a slighter average variance explained (ie, 0.49) was < 0.50, implying that all domains converged appropriately to validity.
Transforming Ordinal Responses to Interval Logit Scores
Rasch modeling, which estimates the mental health and perception of the emotional labor of RTs, was performed to transform ordinal responses into interval logit scores and to conduct statistical analyses. We observed that all mean-squares of infit and outfit ranged from 0.5 to 1.5 (see the supplementary materials at http://www.rcjournal.com), indicating that all subscales fit the Rasch model with a one-dimensional latent construct rather well.
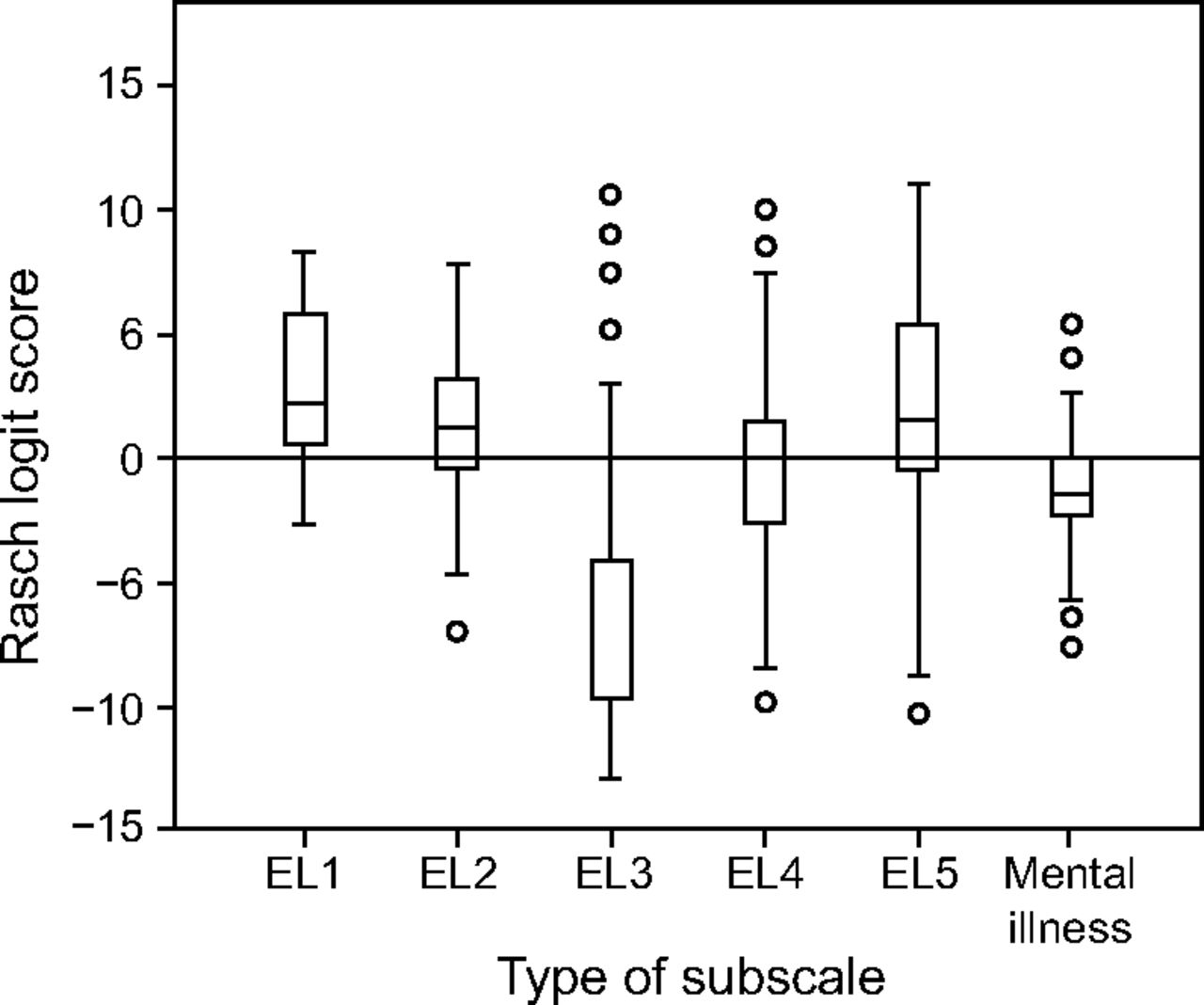
The distributions for each subscale are shown in Figure 1 using box plots. Most RTs with low logits (< 0) were mentally healthy. Similarly, RTs appeared to be healthy on the subscale of interaction extent. The higher scores in Figure 1 indicated that more RTs disagree on the subscales of basic emotional expression, superficial emotional control, and deep emotion camouflage.

Scales of mental health and other subscales for emotion labor using Rasch logit scores. EL = emotional labor.
To inspect the risk factors of mental health derived from the emotional labor subscales and demographic characteristics of RTs in Taiwan, the differences in median scores among the groups were examined, and nonparametric tests were performed (see the supplementary materials at http://www.rcjournal.com). Only 4 demographic characteristics (ie, hospital type, work tenure, RT hierarchy, and weekly work hours) were present as potential risk factors for poor RT mental health. Nonetheless, only age and RT hierarchy influenced the 2 subscales of interaction extent and emodiversity extent (see the supplementary materials at http://www.rcjournal.com).
Risk Factors Influencing the Mental Health of RTs
To extract the key risk factors substantially influencing the mental health of RTs, we performed multiple regression analysis when the 4 potential factors of demographic characteristics and 5 subscales of emotional labor were involved in the model. After a series of pairwise comparisons of the risk factors with the highest insignificant type 1 error (ie, > 0.05), 4 risk factors were retained in the model: basic emotional expression, superficial emotional control, emodiversity extent, and weekly work hours (see Table 2).
Multiple Regression Analysis of Risk Factors of Mental Illness for Respiratory Therapists
It is worth noting that the 2 subscales of basic emotional expression and superficial emotional control presented a negative relationship with mental health (Table 2), indicating that healthy RTs in Taiwan disagree with the organizational stipulations of proper interaction attitudes toward patients.
An App for Assessing the Mental Health of RTs
An app was specifically developed to help RTs examine their mental health at work based on the 32 items extracted from the exploratory factor analysis in this study (Table 1). Readers are invited to check our online videos29,35 to see a video about the app's intention and operational process for practicing it on their own. A total of 32 eligible items were included in the app. The results with Rasch logit scores on each subscale are automatically calculated by the app and displayed on a user's smartphones. This information could help RTs seek mental health consultations at an earlier stage. It is worth noting that the app is available for RTs to use in the future, but it is limited to RTs in Taiwan because these 32 items were extracted from this study.
Discussion
Mental problems are situations of the mind that affect daily functioning. In this study, the 4 factors influencing the mental health of RTs in Taiwan were basic emotional expression, superficial emotional control, emodiversity extent, and weekly work hours (Table 2). The perceptions of emotional labor on a 5-point Likert scale for nurses were higher than that for the RTs who participated in this study, indicating that RTs are less burdened by the organizational regulations of proper interaction attitudes toward patients.36,37
Although few RTs with mental health problems were found in this study (Fig. 1), chiefs and administrators should frequently and aggressively work to safeguard the mental health of RTs at work. Doing so ensures that quality of care is maintained amid the complexity of the hospital environment. Common situations (eg, sleep disturbance, fatigue, limited social interaction, family alienation, social adaptation impact, and requirements of emotional expression) that can easily lead to poor mental and physical health of RTs in critical care units were elucidated.38
Emotional labor reportedly influences the development of poor mental health in the workplace.20,22 Our findings regarding basic emotional expression, superficial emotional control, and emodiversity (ie, emotional diversity) were highly and positively correlated with mental health, similar to the findings of Lee et al,8 and are worthy of further investigations in other countries and regions, as well as other disciplines.
Indregard et al39 reported that health care providers and social workers who frequently experience emotional dissonance had higher levels of exhaustion and mental distress, indicating that health care workers are at high risk of mental health disorders or illness. Furthermore, some effects on emotional health were reported, such as superficial emotional control, emotional expression, emotional expression-incited emotion disorder, and interaction extent.39 These should be addressed within the workplace to prevent the development of issues related to mental health issues.8,40
Delgado et al41 stressed that the ability to deal with the conflict of work rights and duty is required for workers who interact with patients and their family members in hospitals. Chen et al42 reported that front-line workers with a strong desire for harmony tend to adopt a more aggressive strategy when confronted with emotional labor to effectively protect themselves from emotional exhaustion. In contrast, other workers experience dissonance between their outward behavior and inner feelings, which likely exhausts their emotional energy. Some effects that correlate with poor mental health need to be avoided or eliminated from workplaces immediately.39,40
Both RT hierarchy and tiered hospitals are significantly related to mental health (see the supplementary materials at http://www.rcjournal.com). These have rarely been reported in the literature. It is worth noting that lower RT position and tiered hospitals were associated with poor mental health among staff (see the supplementary materials at http://www.rcjournal.com). The reason for this difference could be explained by the work environment, such as respiratory care centers and respiratory care wards for RTs in medical centers and regional hospitals, respectively. The former typically have 1 RT per 10 beds versus 1 RT per 30 beds for the latter, resulting in the latter experiencing relatively heavier workloads.
Regarding weekly work hours as a risk factor, a significantly negative relationship was observed with mental health problems, indicating that normal work hours set at 40 h/week improved mental health when compared with the former 46 h/week (ie, more hours per week resulted in poorer mental health; see the supplementary materials at http://www.rcjournal.com).43
The two subscales of basic emotional expression and superficial emotional control presented a negative relationship with mental health, implying that mentally healthy RTs disagree that proper interaction attitudes toward patients are needed. The reasons for this might be that RTs mostly working in the ICU and the emergency department have little interaction with patients compared to other staff (eg, nurses).
We developed an app for individual RTs to aid them in understanding their mental health at work and to enable them to seek mental health consultation at an earlier stage. A video available on YouTube29 provides information about the app's intention and operational process.
This study has some advantages, such as finding the key risk factors of poor mental health (Table 2) and providing an app for the assessment of the mental health of RTs at work (Fig. 1). However, it also has some limitations. First, data were gathered only from RTs in Taiwan, so the findings cannot be generalized to other countries, regions, or disciplines, although they are worth studying further in the future, as are the questionnaire and the methodologies applied in this study.
Second, Rasch analysis was performed to transform ordinal responses into interval logit scores, which overcomes the problem of considering ordinal scores as intervals in statistics. The drawback of Rasch analysis is that it is difficult for general researchers to learn Rasch modeling techniques due to the numerous mathematical formulas are that required to understand and perform modeling using Rasch software and to interpret the results.
Third, other factors might substantially affect personal mental health at work, such as organization support, teamwork, and patient safety culture. Future research should include other essential variables to accurately extract additional important factors regarding the mental health of RTs in the future.
Lastly, we applied exploratory factor analysis and regression analysis to extract key construct factors of the mental health of RTs (Table 1). Although Rasch analysis was performed to examine the subscale forming a one-dimensional construct using mean squares of infit and outfit (see the supplementary materials at http://www.rcjournal.com), confirmatory factor analysis is suggested to verify the relationship between variables (ie, mental health problems and key influential factors) in the future.
Conclusions
Four risk factors influencing the mental health of RTs at work were verified. Based on the factor structure of the emotional labor and mental health questionnaire and 32 eligible items, an app was developed for RTs to evaluate their own mental health status at work. A video is also available online, where the statistics used in this study are displayed. The app is also demonstrated in the video. Readers are invited to watch the video for details about the study process, data arrangement, and the presentation of results.
RTs are not only trained in cardiopulmonary care but they also specialize in the care of people with pulmonary diseases. They are on the front line in respiratory care (particularly during the global COVID-19 pandemic)44 and work with physicians to help patients survive, resulting in concerns regarding their mental health. RTs with mental health problems can pursue appropriate consultations with mental health specialists at an earlier stage based on the mental health assessment done on their smartphones. However, more relevant studies related to the online assessment of the mental and physical health of RTs are encouraged.
Acknowledgments
We thank the participating respiratory therapist in completing the questionnaires so that the study could be completed successfully.
Footnotes
- Correspondence: Yu-Hua Yan PhD, Department of Hospital and Health Care Administration, Chia Nan University of Pharmacy and Science, No.1, Changda Rd.,Gueiren District, Tainan City, Taiwan. E-mail: 2d0003{at}mail.tmh.org.tw
Supplementary material related to this paper is available at http://www.rcjournal.com.
The authors have disclosed no conflicts of interest.
- Copyright © 2021 by Daedalus Enterprises





{kind=link}