

Abstract
BACKGROUND: Spirometry results can yield a diagnosis of normal air flow, air flow obstruction, or preserved ratio impaired spirometry (PRISm), defined as a reduced FEV1 or FVC in the setting of preserved FEV1/FVC. Previous studies have estimated the prevalence of PRISm to be 7–12%. Our objective was to examine the prevalence of PRISm in a spirometry database and to identify factors associated with PRISm.
METHODS: We performed a retrospective analysis of 21,870 spirometries; 1,616 were excluded because of missing data or extremes of age, height, or weight. We calculated the prevalence of PRISm in prebronchodilator and postbronchodilator pulmonary function tests. Subsequently, we calculated the prevalence of PRISm by various age, race, body mass index, and diagnosis categories, as well as by gender and smokers versus nonsmokers. Finally, in the subset of the cohort with FEV1 < lower limit of normal, we performed a multivariable logistic regression analysis to identify factors associated with PRISm.
RESULTS: We identified 18,059 prebronchodilator spirometries, and 22.3% of these yielded a PRISm diagnosis. This prevalence remained stable in postbronchodilator spirometries (17.7%), after excluding earlier pulmonary function tests for subjects with multiple pulmonary function tests (20.7% in prebronchodilator and 24.3% in postbronchodilator), and when we limited the analysis to prebronchodilator spirometries that met American Thoracic Society criteria (20.6%). The PRISm prevalence was higher in subjects 45–60 y old (24.4%) and in males (23.7%) versus females (17.9%). The prevalence rose with body mass index and was higher for those with a referral diagnosis of restrictive lung disease (50%). PRISm prevalence was similar between races and smokers versus nonsmokers. In a multivariable analysis, higher % of predicted FEV1 (odds ratio 1.51, 95% CI 1.42–1.60), body mass index (odds ratio 1.52, 95% CI 1.39–1.68), and restrictive lung disease (odds ratio 4.32, 95% CI 2.54–7.57) were associated with a diagnosis of PRISm. Smoking was inversely associated (odds ratio 0.55, 95% CI 0.46–0.65) with PRISm.
CONCLUSIONS: In a spirometry database at an academic medical center, the PRISm prevalence was 17–24%, which is higher than previously reported.
- preserved ratio impaired spirometry (PRISm)
- chronic obstructive pulmonary disease
- lung volume measurements
- plethysmography
- respiratory function tests
- spirometry
Introduction
Abnormal nonobstructed spirometry, known as preserved ratio impaired spirometry (PRISm) or restrictive spirometry, occurs in 7–12% of the general population.1–3 Among smokers in the general population with at least 10 pack-years of cigarette smoking who undergo spirometry after bronchodilator use, 12.5% have PRISm.4
PRISm is associated with increased respiratory symptoms, respiratory exacerbations, and mortality.3–5 Unlike obstructive spirometry, PRISm does not indicate a specific lung disease. Subjects with PRISm represent a heterogeneous population with a wide range of lung function impairment and percent of radiographic emphysema.4 PRISm often requires further diagnostic investigation to identify the underlying lung disease.
Although the prevalence of PRISm has been studied in research cohorts in the general population and in smokers, the prevalence of PRISm in everyday clinical life is understudied. In a single-center study, 9.5% of all post-bronchodilator pulmonary function tests (PFTs) had FEV1 and FVC below the lower limit of normal while FEV1/FVC, diffusing capacity for carbon monoxide, and total lung capacity (TLC) above the lower limit of normal.6 In our previous work, which included only PFTs that met the American Thoracic Society criteria for acceptability and repeatability, we reported that 37.4% of all pre-bronchodilator spirometries and 57% of abnormal spirometries had PRISm.7
Smoking exposure, high body mass index, and reduced TLC have been associated with PRISm among a cohort of smokers without interstitial lung disease.8 The factors associated with PRISm in the clinical setting are not known. We hypothesized that the prevalence of PRISm in PFTs performed for clinical purposes is high. To investigate our hypothesis, we assessed the prevalence of PRISm in spirometries before and after bronchodilator use in our PFT labs that met the American Thoracic Society (ATS) criteria. We examined the association of PRISm with demographics, lung volume measurements, and referral diagnosis for the PFTs.
QUICK LOOK
Current Knowledge
Preserved ratio impaired spirometry (PRISm) is a spirometric pattern associated with respiratory symptoms and increased mortality. Individuals with PRISm represent a heterogenous group of diseases. It is possibly underdiagnosed and underappreciated. PRISm is likely more prevalent in patients in academic medical centers and in larger cohorts of medically complex patients.
What This Paper Contributes to Our Knowledge
PRISm was more prevalent in our spirometry database compared to previously reported prevalence in the general population. It remained very stable in several subanalysis groups. Individuals with PRISm represent a heterogenous population that cannot be fully explained by obesity, interstitial lung disease (or other restrictive lung disease) or differences in race.
Methods
Data Collection
We conducted a retrospective analysis of data from PFTs performed at the University of Iowa Hospital from 1997 to 2018. The institutional review board approved the study protocol (201810837). After prebronchodilator spirometry, lung volumes were measured with plethysmography without bronchodilator. Postbronchodilator spirometry was performed 10 min after administration of 3 puffs of albuterol using a pressurized metered-dose inhaler and spacer. The PFT cohort in this is from the largest academic medical center in the state of Iowa and a referral center for interstitial lung disease, cancer, heart failure, and complex surgical and transplant patients.
We included subjects > 18 y old. We excluded PFTs with no available reference values in NHANES III,9 including PFTs of patients from American Indian (n = 3), Asian (n = 164), or mixed race (n = 13); PFTs of patients > 80 y old (n = 1,031); and PFTs of patients with height < 140 cm (n = 58), > 217 cm (n = 1), and with weight < 35 kg (n = 25). We collected PFT measurements as well as age, sex, height, race, and referral diagnosis from the PFT database in our PFT lab. Smoking status was retrieved from the electronic medical records.
Because the prevalence of PRISm may vary depending on whether pre- or postbronchodilator spirometry was used and whether the spirometry met the ATS criteria, we assessed PRISm prevalence in the following groups: (1) all prebronchodilator and postbronchodilator spirometries, (2) unique PFTs for each individual (if there were multiple PFT for a single individual, we kept the most recent), and (3) only prebronchodilator spirometries that met the ATS criteria.
Definitions and Outcomes
PRISm was defined as FEV1/FVC ≥ lower limit of normal and FEV1 < lower limit of normal using reference values from the third National Health and Nutrition Examination Survey (NHANES III).9 Obstruction was defined as FEV1/FVC < lower limit of normal, and normal spirometry was defined as FEV1/FVC ≥ lower limit of normal and FEV1 ≥ lower limit of normal. Referral diagnoses were divided into 5 categories based on codes from the International Classification of Diseases, Tenth Revision: interstitial lung disease, restriction, obstructive lung diseases, other respiratory disease, miscellaneous, and none when none was available. Other respiratory diseases were defined as those respiratory diseases or conditions that do not fall into the obstructive lung disease or interstitial lung disease category (eg, dyspnea, hypoxemia, cough, neuromuscular disease). No respiratory diseases or conditions were defined as miscellaneous. Lung volume was categorized into the following groups: (1) restriction defined as TLC < lower limit of normal and RV/TLC < upper limit of normal; (2) air trapping or hyperinflation defined as TLC > upper limit of normal or RV/TLC > upper limit of normal; (3) unclassified, defined as TLC < lower limit of normal and RV/TLC > upper limit of normal; and (4) normal, defined as TLC > lower limit of normal and TLC < upper limit of normal combined with RV/TLC < upper limit of normal. Severity of lung function impairment among PRISm was categorized into mild (FEV1 50–80% of predicted), moderate (FEV1 30–50% of predicted), and severe (FEV1 < 30% of predicted).
Statistical Analysis
We stratified PFTs by age, race, sex, body mass index, smoking status, lung volume group, and diagnosis. We compared the prevalence of PRISm between groups using the Fisher exact test or the chi-square test when appropriate. We assessed concordance between spirometries before and after bronchodilator use to categorize spirometries as mormal, obstruction, or PRISm using κ statistics. To identify factors associated with PRISm among patients with abnormal spirometry, we created a subset that included only patients with FEV1 < lower limit of normal (ie, normal spirometries were excluded). Univariate comparisons were then performed using the Fisher exact test for categorical variables and a Student t test or Wilcoxon rank-sum test for normal and non-normal continuous variables, respectively, to identify variables associated with PRISm. Variables with a univariate P < .05 were considered candidates in the multivariable regression model. Variables were selected using a stepwise backward elimination to minimize the Akaike information criterion.10
In a sensitivity analysis, we calculated the prevalence of PRISm among spirometries that met the ATS criteria as pre-bronchodilator FEV1/FVC ≥ lower limit of normal and FVC ≤ lower limit of normal. We used the R software package for all statistical analysis (http://www.r-project.org).
Results
We identified a total of 21,870 PFTs. We excluded 1,211 records of patients > 80 y old or patients who were not white, African-American, or Hispanic. We also excluded 84 PFTs for extremes of height or weight, and 321 patients with no available spirometry (eg, PFT records included only lung volumes or the diffusing capacity for carbon monoxide). After these exclusions, a total of 20,254 records remained. Figure 1 shows the CONSORT diagram.

Flow chart. PFT = pulmonary function tests; ATS = American Thoracic Society.
Of 20,254 PFTs that had at least a pre-bronchodilator or a post-bronchodilator spirometry, 18,059 records had prebronchodilator spirometries, and 8,494 records had postbronchodilator spirometries. The prevalence of PRISm was 22.3% (4,030) and 17.7% (1,507) in pre- and postbronchodilator spirometries, respectively. When we limited the analysis to unique subjects, we identified 9,988 records, with 9,768 prebronchodilator and 4,567 postbronchodilator spirometries. Of the 9,768 prebronchodilator spirometries, 2,031 (20.7%) were PRISm. Of 4,567 postbronchodilator spirometries, 1,110 (24.3%) yielded PRISm.
Characteristics of Spirometries That Met ATS Criteria
Among the spirometries that met ATS criteria (6,494), the prevalence remained stable when we limited the analysis to unique records that met the ATS criteria in the prebronchodilator spirometries (1,342 out of 6,494, 20.6%).
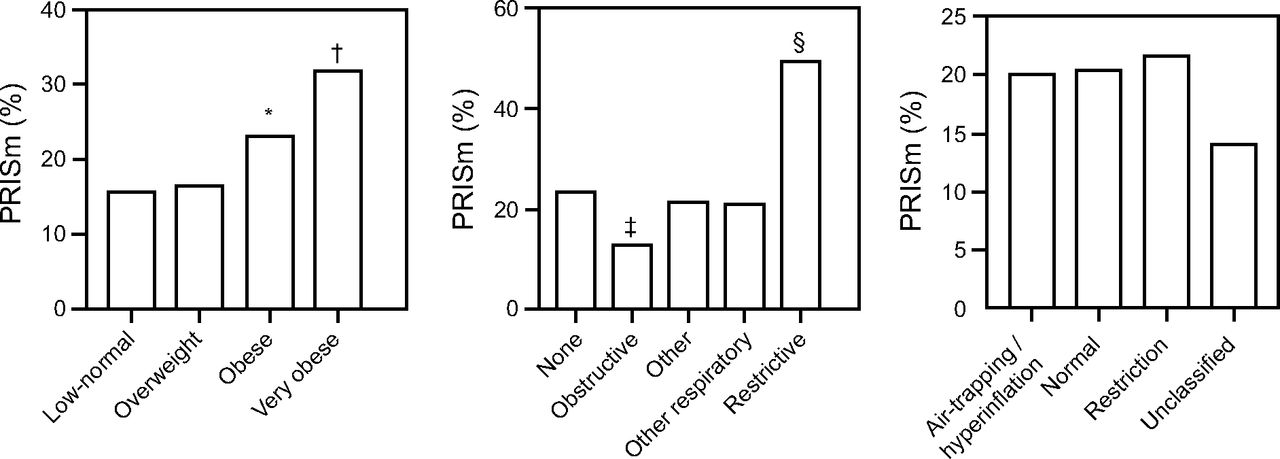
Table 1 shows the baseline characteristics of subjects who met ATS criteria. Figure 2 and Figure 3 show the prevalence of PRISm in several subgroups. The PRISm prevalence was higher in subjects 45–60 y old and in males versus females. The prevalence also rose with body mass index and with a referral diagnosis of restrictive lung disease (50%). PRISm prevalence was similar between races (19.8% in Hispanics, 20.9% in whites, 16.9% in African-Americans) and smokers (20.8%) versus nonsmokers (20.5%). We then examined the severity of lung function among PRISm based on FEV1: 1,043 (77.7%) had mild lung function impairment (FEV1 50–80%), 261 (19.4%) had moderate lung function impairment (FEV1 30–50%), and 38 (2.8%) had severe lung function impairment (FEV1 < 30%).

Subgroup analysis of preserved ratio impaired spirometry (PRISm) based on age, sex, and smoking status. * P < 0.01 between 45–60 year old and all other age groups, † P < 0.01 between female and male sex.

Subgroup analysis of preserved ratio impaired spirometry (PRISm) based on body mass index, diagnosis category, and lung volumes. * P < 0.01 between obese and low-normal/overweight, † P < 0.01 between very obese and all other weight groups, ‡ P < 0.01 between obstructive and none, § P < 0.01 between restrictive and all other PFT patterns.
Baseline Characteristics of PFTs That Met American Thoracic Society Criteria
Using 2,930 records that had both pre- and postbronchodilator spirometries available, the agreement between pre- and postbronchodilator spirometry was poor with κ = 0.125 (Table 2). The prevalence of PRISm was 19.6% and 23.2% in pre- and postbronchodilator spirometries, respectively. When we defined PRISm as prebronchodilator FEV1/FVC ≥ lower limit of normal and FVC ≤ lower limit of normal, the prevalence of PRISm was 22.3% (1,448 of 6,494).
Agreement Between Pre- and Postbronchodilator Spirometry
Table 3 shows factors which were found to be associated with PRISm among those with abnormal spirometry (n = 2,909). In multivariable analysis, higher FEV1 percent of predicted in 10% increments (odds ratio 1.51, 95% CI 1.42–1.60), body mass index in increments of 10 kg/m2 (odds ratio 1.52, 95% CI 1.39–1.68), and restrictive lung disease (odds ratio 4.32, 95% CI 2.54–7.57) were associated with a diagnosis of PRISm. Smoking was inversely associated with PRISm (odds ratio 0.55, 95% CI 0.46–0.65).
Factors Associated With PRISm Among Individuals With Abnormal Spirometries
Discussion
Our results indicate that the prevalence of PRISm was 17–24% in a PFT lab dataset from an academic medical center. The prevalence remained relatively stable in several subanalysis groups, including a subanalysis of postbronchodilator spirometries after excluding earlier PFTs for subjects with multiple PFTs and a subanalysis that included only prebronchodilator spirometries that met ATS criteria. Among those with abnormal lung function, obesity and restrictive lung disease were associated with PRISm. Poor lung function (ie, lower FEV1) and smoking were inversely associated with PRISm.
Several studies assessed the prevalence of PRISm in the general population. In the NHANES I cohort, which included prebronchodilator spirometries from the general population, the prevalence of spirometries with FVC < 80% and FEV1/FVC > 0.7 was 9.2%.2 Using data from the ARIC study, Mannino et al3 noted that 7.1% of all subjects had prebronchodilator FVC < 80% and a prebronchodilator FEV1/FVC > 0.7. Of abnormal spirometries, 16% had PRISm. In the Tucson epidemiological study, Guerra et al1 reported the PRISm prevalence to be 12%. In that study, 46% of abnormal spirometries were PRISm. In the COPDGene cohort, which included only smokers and excluded patients with interstitial lung disease, the prevalence was 12.3%.5 In this study, we extended the literature by showing that the prevalence of PRISm was 17–24% in a PFT lab cohort at an academic medical center. The prevalence of PRISm was higher than in general-population studies.1–3 However, Jankowich et al11 reported a prevalence of 19.9% in an African-American population in Mississippi, which corroborated previous studies that reported higher PRISm in African-Americans.8,12
Prior reports have used variable definitions for PRISm, such as FVC < 80%1–3 or FEV1 < 80% combined with an FEV1/FVC ≥ 0.7.4,13 FEV1 and FVC are concomitantly reduced, whereas an isolated reduction in FEV1 or FVC is infrequent.7,14 Iyer et al14 reported that, among all abnormal nonobstructed spirometries, 85.5% had both reduced FEV1 and FVC, whereas 11.2% had only low FEV1, and 3.3% had isolated low FVC. Our previous work indicated that isolated reduction in FEV1 was only 4.7% of all abnormal nonobstructed spirometries.7 In this cohort, prevalence did not vary whether PRISm was defined as FVC ≤ lower limit of normal with FEV1/FVC ≥ lower limit of normal, or as FEV1 ≤ lower limit of normal with FEV1/FVC ≥ lower limit of normal. Other studies used spirometry before bronchodilator use,1–3,11 and others used spirometry after bronchodilator use.4 Although the prevalence of PRISm in our study is similar regardless of whether spirometry was done before or after bronchodilator use, Table 2 shows their agreement being poor (κ = 0.125). Previous COPD studies have reported that pre-and postbronchodilator spirometries have similar predictive values based on correlation with clinical outcomes.10,15 Further research should assess the correlation of PRISm based on pre- and postbronchodilator spirometries with clinical outcome to assess whether postbronchodilator offers better results.
PRISm is often considered to be a result of obesity. The body mass index of individuals with PRISm is higher than that of smokers with normal spirometry or COPD.8 This is in agreement with our findings. Nevertheless, a landmark study by Jones and Nzekwu16 indicated that, although body mass index is inversely associated with FVC, obesity is unlikely to reduce FVC below the lower limit of normal in individuals with no respiratory disease. Among subjects undergoing preoperative evaluation for bariatric surgery with a body mass index at least of 35 kg/m2, only 3% had an FVC < lower limit of normal.17
Further, PRISm has been considered equivalent to restrictive respiratory disease. Although it is likely true that PRISm occurs in interstitial lung diseases, overall the prevalence of interstitial lung disease is very low, and it likely represents only a very small proportion of PRISm. Moreover, the prevalence of PRISm in the COPDGene cohort, which excluded interstitial lung disease, is 9–12.5%.4
If neither obesity nor interstitial lung disease are responsible for the larger proportion of PRISm, then what causes PRISm? Individuals with PRISm represent a heterogenous population. In smokers with PRISm, body mass index ranges from 17.2 to 53.8 kg/m2, FEV1 ranges from 44% to 79%, and radiographic emphysema ranges from 0.01% to 11.43%.1 A proportion of PRISm may be related to abnormal lung growth in early life. Seventeen percent of the general population had PRISm in their early 30s.18 Nevertheless, the most common respiratory diseases that can cause lung function impairment are obstructive lung diseases like asthma and COPD. It is very likely that obstructive lung diseases are responsible for most PRISm cases. Increased body mass index in combination with obstructive lung disease may result in abnormal spirometry with preserved FEV1/FVC. O'Donnell and colleagues19 reported that obesity results in increased FEV1/FVC in subjects with COPD. In a recent study, Wijnant and colleagues13 noted that half of the PRISm subjects in the general population developed obstructive spirometry after a few years. In the Lovelace cohort, which included smokers from the general population (80% women), Sood et al20 reported that a proportion of subjects with COPD may have PRISm in follow-up spirometries and, vice versa, a proportion of PRISm individuals may have COPD. There is spirometric pattern change between COPD and PRISm over time.4,20 This variation occurs mostly in mild and moderate lung impairment, given that there are no PRISm individuals with FEV1 < 44% in heavy smokers with no interstitial lung disease.8 In our cohort, increasing FEV1 percent of predicted was inversely associated with PRISm and confirms that.
Table 2 shows the poor agreement in our database based on whether pre- or postbronchodilator spirometry is used (κ = 0.125). Of 573 prebronchodilator PRISm, 205 returned to normal after bronchodilator use (likely an increase in both FEV1 and FVC), suggesting a possible early obstructive (and partially reversible) test; 66 became obstructive, likely due to predominant bronchodilator response in FVC, which is common in COPD.21 These findings suggest that 47% (271 of 573) of these prebronchodilator PRISm may have early or mild obstructive disease that would only be revealed if these patients were given a bronchodilator. In the reciprocal analysis, of 710 postbronchodilator PRISm, 101 had prebronchodilator obstruction that normalized after bronchodilator use, indicating a larger increase in FEV1 compared to FVC and resulting in a normal FEV1/FVC, which is typically seen in asthma (eg, flow response). Of 710 postbronchodilator PRISm, 307 had normal prebronchodilator spirometry. This might be explained by poor postbronchodilator effort, or it could be due to paradoxical bronchodilator response.22 The above results suggest that both pre- and postbronchodilator should be considered even when prebronchodilator test is not obstructive because administration of a bronchodilator might give more information on the pulmonary physiology.
Our study has several limitations. First, the use of retrospective data and using referral diagnosis by International Classification of Diseases codes might have biased the statistical analysis. Second, our spirometry data are spread over more than 20 years, from 1997 to 2018, with different spirometers and plethysmographs being used. Third, our study only looked at the prevalence of PRISm, and we have neither clinical follow-up data about the subjects nor occupational or environmental exposure history. Fourth, the PFT cohort in this study is from an academic medical center, which is different from a community hospital; our study sample is racially homogenous with 92.9% being white, which is a good representation of that proportion of the population of Iowa (90.1% white according to the 2010 Census23), but it may limit the generalizability of our study. Fifth, our PFT lab performed the postbronchodilator spirometry 10 min after 3 puffs of albuterol, which may have led to an underestimation of bronchodilator response. These limitations do not undermine the strengths of our study, ie, the large sample size, the fact that all PFTs were performed in the same lab, and the reproducibility in several subgroup analysis. The fact that different spirometers and plethysmographs were used across 20 years increases our work's external validity.
Conclusions
PRISm is a spirometric pattern associated with respiratory symptoms and increased mortality. This study indicates that the prevalence of PRISm among subjects referred to a PFT lab in an academic medical center (17–24%) is much higher than the prevalence in the general population. Although there is a discordance between pre- and postbronchodilator spirometry, the prevalence of PRISm when prebronchodilator spirometry was used is similar to the prevalence when postbronchodilator spirometry was used. Due to the poor agreement between spirometry before and after bronchodilator use, bronchodilators should be used to help distinguish between different pulmonary physiologies. Obesity and restrictive lung disease are associated with PRISm, while poor lung function and smoking are inversely associated with PRISm. Further research is needed to examine a diagnostic approach that will help identify the underlying diseases or conditions associated with PRISm and potential treatments.
Footnotes
- Correspondence: Spyridon Fortis MD, UIHC Internal Medicine, 200 Hawkins Drive, C33 GH, Iowa City, IA 52242. Email: spyridon-fortis{at}uiowa.edu
The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States Government.
Dr Fortis is supported by the Department of Veterans Affairs (Award # 14380), the Comprehensive Access and Delivery Research and Evaluation Center (CIN 13-412), and has received grants from the American Thoracic Society, and Fisher & Paykel. The other authors have disclosed no conflicts of interest.
- Copyright © 2021 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}