

Abstract
BACKGROUND: The ventilatory ratio (VR) is a simple index of ventilatory efficiency and dead space. Because increased dead space and high ventilatory demands impose a limitation to unassisted ventilation, and may predispose patients to injurious strong efforts during assisted ventilation, evaluation of the VR could provide helpful information during weaning. We hypothesize that there is a threshold of VR associated with tolerance of unassisted breathing.
METHODS: In a retrospective analysis, we included subjects ventilated in a control mode for at least 24 h, who were successfully liberated from mechanical ventilation, without use of noninvasive ventilation, and discharged alive from the ICU. We focused on the successful weaning attempts (the last, if more than one was performed) and evaluated the VR at the beginning and at the end of the assisted ventilation period.
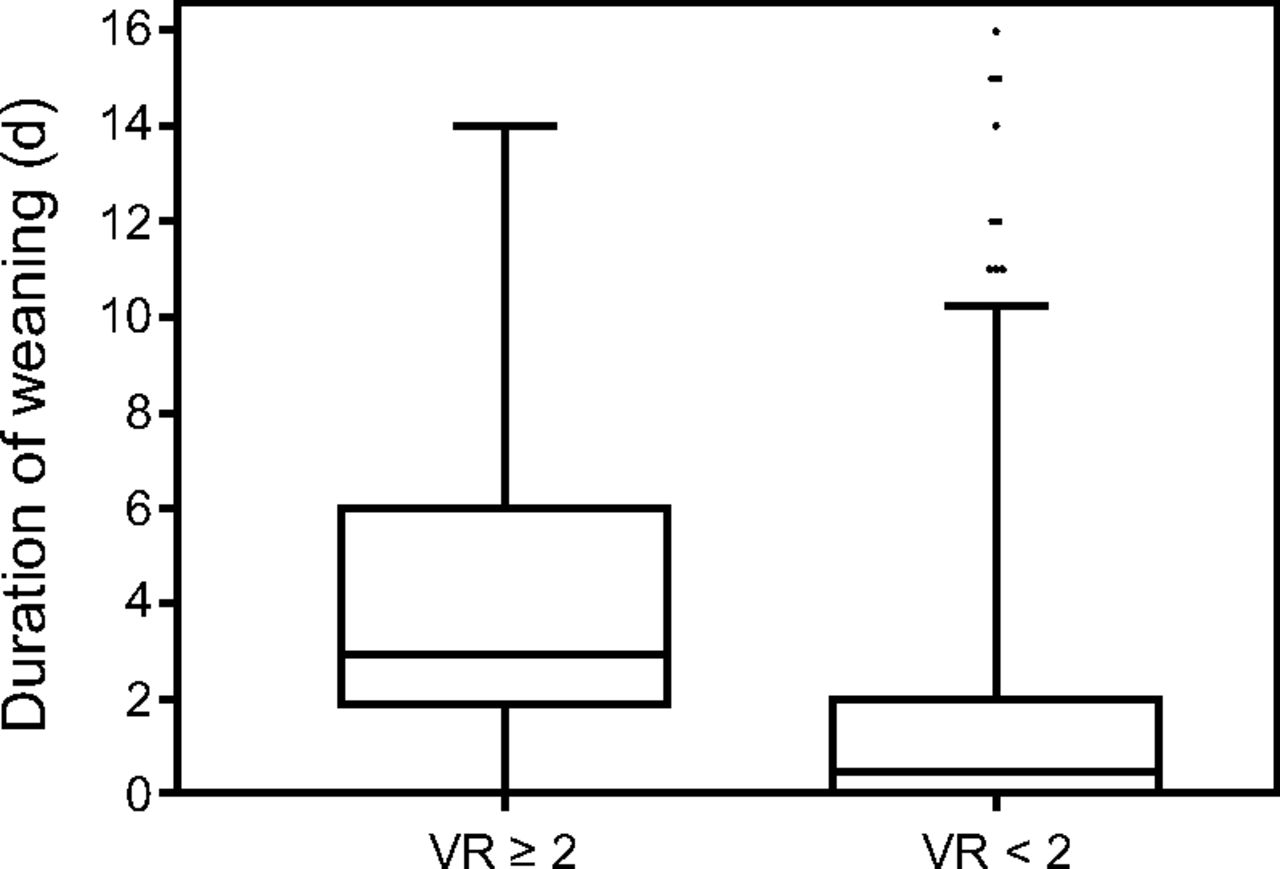
RESULTS: We examined 2,000 medical records and included in our analysis 572 subjects (age: 68 y, R5-95 = 25–85, 68% male) with main admission diagnosis of respiratory failure (23%), sepsis (11%), brain injury (34%), and postoperative (14%). The VR at the beginning and the end of the assisted ventilation period was 1.5 (R5-95 = 1–2.1) and 1.4 (R5-95 = 1–2), respectively. The median duration of assisted ventilation in subjects with a VR ≥ 2 at the beginning of the assisted ventilation period was 3 d (R5-95 = 0–14 d), significantly longer than in those with a VR < 2, 0.5 d (R5-95 = 0–8 d, P < .001).
CONCLUSIONS: Successful liberation from assisted ventilation was associated with a VR < 2. A VR > 2 was associated with longer duration of weaning. The VR could be used as an additional tool to facilitate the decision-making process during weaning.
Introduction
The ventilatory ratio (VR) is a simple index of ventilatory efficiency and dead space, shown to be independently associated with prolonged duration of mechanical ventilation and increased ICU and hospital mortality in ARDS patients.1-5 The VR is a unitless variable calculated as the ratio of the observed minute ventilation (V˙E) and arterial carbon dioxide pressure ( ) product over the predicted V˙E and
) product over the predicted V˙E and  product: VR = V˙E (mL) ×
product: VR = V˙E (mL) ×  (mm Hg)/predicted V˙E × 37.5 (mm Hg), using for predicted V˙E the formula predicted V˙E = 100 mL/kg × ideal body weight (kg).1
(mm Hg)/predicted V˙E × 37.5 (mm Hg), using for predicted V˙E the formula predicted V˙E = 100 mL/kg × ideal body weight (kg).1
The VR is affected by dead space (VD) and VD/VT, V˙/Q˙ mismatch, and shunt.6,7 The breathing pattern, tidal volume (VT), and respiratory frequency (f) also affect the VR, as different combinations of VT and f may result in the same V˙E but different VD/VT. Despite the assumptions used in the calculation of predicted V˙E, the VR is an informative and simple-to-obtain index of ventilatory efficiency at the bedside. A high VR indicates increased ventilatory demands. Ventilatory demands are among the 3 factors affecting the patients’ ability to sustain unassisted breathing, along with respiratory system mechanics and muscle strength, and thus affect the weaning process.8 As increased ventilatory demands may impose a limitation to unassisted ventilation, and predispose patients to injurious strong efforts during assisted ventilation,9-11 evaluation of the VR could provide helpful information during weaning.
We hypothesize that there is a threshold of VR associated with tolerance of unassisted breathing. As a first step to explore this hypothesis, we evaluated the range of VR observed during assisted spontaneous breathing in patients successfully liberated from mechanical ventilation.
QUICK LOOK
Current Knowledge
The VR is a simple index of ventilatory efficiency and dead space, shown to be independently associated with adverse outcome in ARDS patients. A high VR indicates increased ventilatory demands and may impose a limitation to spontaneous breathing and predispose patients to injurious strong efforts during assisted patient triggered ventilation, suggesting that evaluation of the VR could provide helpful information during weaning.
What This Paper Contributes to Our Knowledge
In this retrospective study of critically ill subjects from a mixed adult ICU during weaning, successful liberation from patient triggered ventilation was associated with a VR < 2. A VR > 2 was associated with longer duration of weaning and ICU length of stay.
Methods
A retrospective analysis of the last 2,000 medical records of critically ill patients admitted at the University Hospital of Heraklion ICU (4-y period) was performed, approved by the local ethics committee. In the analysis, we included subjects ventilated in a control mode for at least 24 h, who were successfully liberated from mechanical ventilation, without use of noninvasive ventilation, and discharged alive from the ICU. We excluded patients with chronic hypercapnic respiratory failure, and shorter than 152, due to a limitation of the ideal body weight equation. During the analyzed period, subjects were ventilated on either pressure support or proportional assist ventilation (PAV+) mode, and weaning was performed using our previously described weaning protocol12 with minor modifications. Arterial blood gas analysis was routinely performed 6 times daily and after any change in mode of ventilation. We evaluated the VR using the  and V˙E of the arterial blood gas (ABG) analysis obtained at the beginning and the end of the weaning period as shown in Figure 1 at the beginning (last ABG in control mode) and the end (last ABG in assisted mode) of assisted ventilation and the first only in CPAP among unassisted modes (because V˙E is not measured in T-piece or after extubation). We focused on the successful weaning attempts, and only the last prior to ICU discharge, if more than one was performed in a subject. The time period between the beginning and the end of ventilation in assisted mode is reported as duration of weaning (in d). Subjects placed on CPAP or T-piece directly from control mode were considered to have 0 d of weaning, and because not all subjects were placed on assisted ventilation or CPAP prior to extubation or T-piece, the number of observations in the end of assisted and CPAP mode is smaller than those of the last in control mode. We computed the VR as previously described,1 using subjects’ height measured on admission to estimate the ideal body weight. We also calculated the ideal body weight corrected for the age-related height loss,13 because in our ICU height is measured on admission, and computed a corrected VR. VR and corrected VR were calculated according to the equations:
and V˙E of the arterial blood gas (ABG) analysis obtained at the beginning and the end of the weaning period as shown in Figure 1 at the beginning (last ABG in control mode) and the end (last ABG in assisted mode) of assisted ventilation and the first only in CPAP among unassisted modes (because V˙E is not measured in T-piece or after extubation). We focused on the successful weaning attempts, and only the last prior to ICU discharge, if more than one was performed in a subject. The time period between the beginning and the end of ventilation in assisted mode is reported as duration of weaning (in d). Subjects placed on CPAP or T-piece directly from control mode were considered to have 0 d of weaning, and because not all subjects were placed on assisted ventilation or CPAP prior to extubation or T-piece, the number of observations in the end of assisted and CPAP mode is smaller than those of the last in control mode. We computed the VR as previously described,1 using subjects’ height measured on admission to estimate the ideal body weight. We also calculated the ideal body weight corrected for the age-related height loss,13 because in our ICU height is measured on admission, and computed a corrected VR. VR and corrected VR were calculated according to the equations:








Time points of ventilatory ratio calculation.
We analyzed 2 subgroups of subjects, those ventilated through an endotracheal tube rather than a tracheostomy, to evaluate the effect of dead-space reduction of tracheostomy on VR, and subjects with acute respiratory failure. In this group, we included subjects admitted in the ICU for acute respiratory failure and subjects having a  /
/ < 200 mm Hg at the beginning of weaning. We also evaluated the effect of mode of assist (pressure support or PAV+) on VR and outcome.
< 200 mm Hg at the beginning of weaning. We also evaluated the effect of mode of assist (pressure support or PAV+) on VR and outcome.
Statistical analysis: The distribution of values was evaluated for normality with Shapiro-Wilk test, and for all parameters the median and R5-95 percentile range are reported. Comparison between groups is performed with Mann-Whitney U test for non-normally distributed data.
Results
From the 2,000 medical records analyzed, we excluded 222 cases of non-critically ill patients admitted for invasive procedures, 708 patients who were either not intubated or ventilated in control mode < 24 h, 369 patients who died in the ICU, 98 patients who were extubated to noninvasive ventilation or discharged on invasive ventilation from the ICU, and 41 patients shorter than 152 cm; hence, 572 subjects were included in the analysis. The median age was 68 y, (R5-95 = 25–85), 68% were male, with main admission diagnoses of respiratory failure (23%), sepsis (11%), brain injury (34%), and postoperative (14%). The median ICU length of stay was 12 d (R5-95 = 4–34), and the duration of mechanical ventilation 8 d (R5-95 = 2–27).
The VR and corrected VR at the beginning and the end of the assisted ventilation period for all subjects are presented in Figure 2A. The upper range of VR values associated with successful liberation from assisted ventilation was 2. As shown in Figure 2B, no significant difference in the distribution or threshold of corrected VR was observed in the subgroups of patients with endotracheal tube or respiratory failure.

A. Ventilatory ratio (VR) and corrected VR for age-related height loss at the beginning and the end of the assisted ventilation period in all subjects; and B. Corrected VR at the beginning and the end of the assisted ventilation period in subjects ventilated through an endotracheal tube and subjects with respiratory failure. The number of observations at each time point was for all subjects 572, 383, 303 for beginning and end of assisted and CPAP, respectively; for subjects with endotracheal tube, 325, 182, 156; and for subjects with respiratory failure, 198, 158, 96, respectively. Boxes represent interquartile range, whiskers the R5-95 range; dots represent outliers, and line is at median.
The median duration of assisted ventilation in subjects with a VR ≥ 2 at the beginning of the assisted ventilation period was much greater than in those with a VR < 2, Figure 3. Similarly, the total duration of mechanical ventilation and the duration of ICU length of stay correlated positively with the VR at the beginning of the assisted ventilation period (Spearman correlation coefficient 0.28 for the duration of mechanical ventilation and 0.24 for ICU length of stay), and it was greater in subjects with a VR ≥ 2 than in those with a VR < 2 (14 vs 8 d and 19 vs 11 d, respectively, P < .001 for both).

The duration of assisted ventilation is shorter when subjects’ VR at the beginning of weaning is < 2 (median 0.5 d) than when VR ≥ 2 (median 3.0 d), P < .001 by Mann Whitney U test.
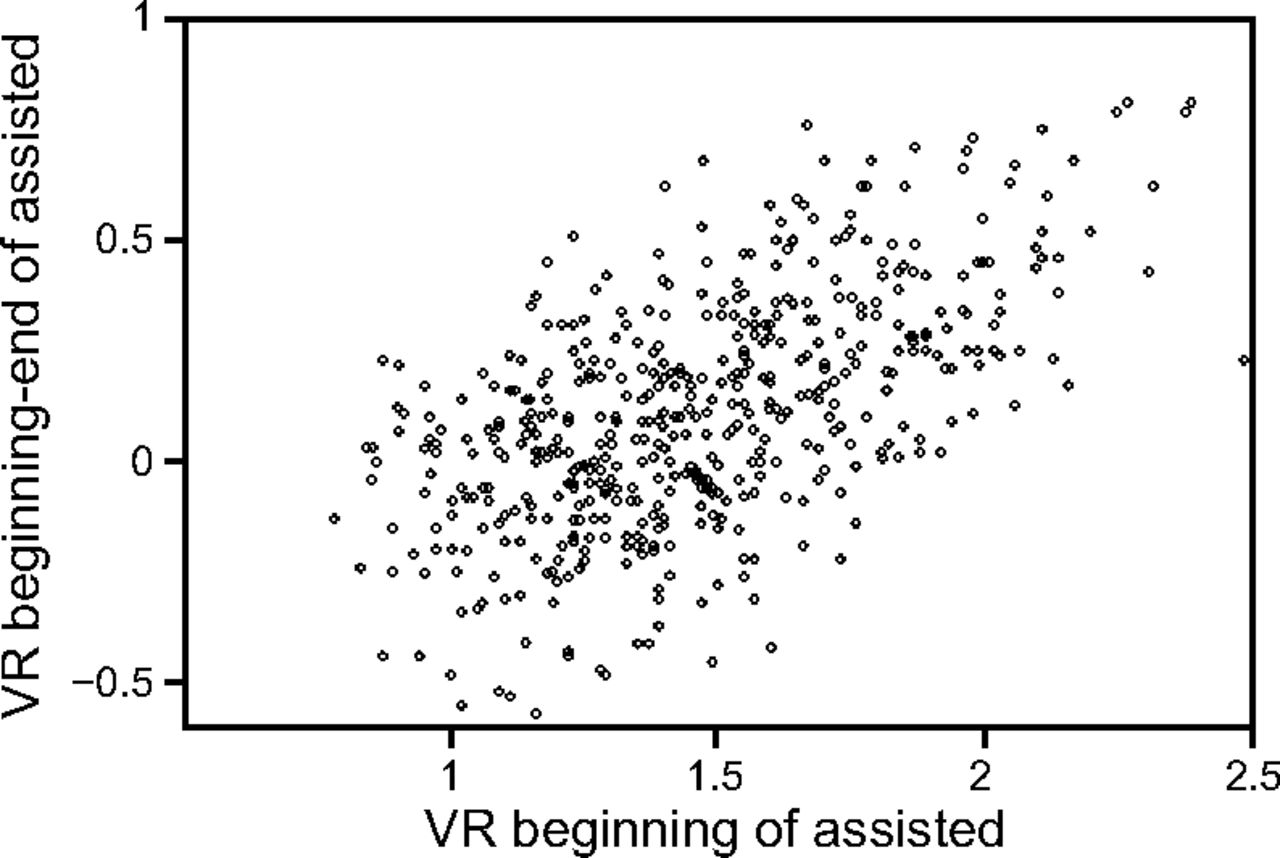
We finally examined the change of VR during the course of weaning. The change of VR during weaning (from beginning to end) varied significantly among subjects (median 0.1, R5-95 = −0.3 to −0 .6), showing improvement in 60% of the subjects. As shown in Figure 4, VR changes varied when the VR at the beginning of weaning was low but always improved when VR was initially > 1.8. There was no difference in the change of VR between patients ventilated with pressure support or PAV+.

Change of VR from the beginning to the end of weaning relative to its initial value. A positive change indicates improvement (decrease) of VR during weaning.
Discussion
In this retrospective analysis, we observed that the VR was always < 2 when subjects were able to maintain unassisted breathing. A high VR at the beginning of weaning was associated with prolonged duration of assisted ventilation and ICU stay.
The VR is a simple index of ventilatory efficiency, as  /
/ is an index of oxygenation. Although the VR has many oversimplifications, similarly to
is an index of oxygenation. Although the VR has many oversimplifications, similarly to  /
/ its simplicity makes it appealing for use in everyday practice to monitor and stratify ventilatory efficiency and risk of weaning failure.
its simplicity makes it appealing for use in everyday practice to monitor and stratify ventilatory efficiency and risk of weaning failure.
The results of this study show that a high VR > 2 is not observed when physicians extubate patients or place them on CPAP or T-piece. A previous study has shown that a high VR on admission was associated with prolonged duration of mechanical ventilation.2 In line with this observation, the results of the present study showed that when the VR was high at the beginning of assisted ventilation a longer duration of assisted ventilation was observed, and subjects were finally liberated from ventilatory assistance only when their VR fell < 2. Clearly, a low VR cannot ensure liberation from mechanical ventilation or successful extubation because it merely indicates ventilatory efficiency and not the adequacy of respiratory muscles to compensate for the present load imposed by abnormalities of the respiratory system mechanics. Yet, a high VR is not compatible with liberation from assisted ventilation but associated with prolonged need for mechanical ventilation and ICU length of stay.
This study has the limitations associated with a retrospective, single-center study. Our findings are likely affected by the weaning protocol used, which, nonetheless, is similar to common practice. The case mix studied also may have affected the results, but the subgroup analysis did not show differences among specific groups of subjects, such as those with respiratory failure. Due to the retrospective nature of the analysis, the impact of VR on the decision making process during weaning could not be evaluated, and the incidence of weaning failure due to increased ventilatory demands and high VR could not be examined.
The VR threshold 2 for unassisted breathing identified in this study could be confirmed in other, larger databases and studied as a tool to facilitate the decision making process during weaning.14,15 For example, initiation of weaning is usually suggested based on improvement of oxygenation and hemodynamic stability. Yet, a VR in control mode much > 2 indicates patients’ ventilatory demands are high; thus, there is a risk for injurious strong inspiratory efforts during assisted ventilation, and closer monitoring of effort or delayed weaning could be considered.9,11,14,15 Therefore, the VR could be incorporated in weaning protocols to complement indices of oxygenation in the identification of readiness to wean. Similarly, the VR could be used to identify patients with increased ventilatory demands at extubation (a VR close to 2) who could be candidates for preventive interventions to avoid extubation failure.
Conclusions
Our findings suggest that the VR is a useful index to monitor patients’ ventilatory efficiency during the weaning process. A high VR is associated with prolonged duration of mechanical ventilation, and a VR < 2 appears to be necessary for unassisted breathing. Therefore, a VR threshold 2 could be used to characterize patients’ ventilatory efficiency for unassisted ventilation and complement the indices of oxygenation in the decision making process during weaning.
Footnotes
- Correspondence: Katerina Vaporidi MD PhD, University of Crete School of Medicine, Voutes Campus, Office 8A4, 70013, Heraklion, Crete, Greece. E-mail: vaporidi{at}uoc.gr
The study was performed at the intensive care unit of the University Hospital of Heraklion, Crete, Greece.
Drs Georgopoulos, Kondili, and Vaporidi disclose relationships with Medtronic. The other authors have no conflicts to disclose.
- Copyright © 2021 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}