

Abstract
BACKGROUND: The number of patients requiring prolonged mechanical ventilation (PMV) is predicted to escalate due to an aging population. International studies on prevalence and resource utilization of this patient group exist, but data are lacking from Scandinavian ICUs, where there is a relatively low number of ICU beds in relation to population. The primary aim was to identify prevalence of admissions requiring mechanical ventilation ≥ 7–21 d and PMV > 21 d, and their use of ICU bed days in Sweden. Secondary aims were to describe patient characteristics and outcomes.
METHODS: We obtained data from the Swedish Intensive Care Registry on admissions age ≥ 18 y mechanically ventilated ≥ 7 d and used open source registry data to calculate the prevalence and use of bed days of admissions ventilated ≥ 7–21 d and PMV > 21 d.
RESULTS: Of the 39,510 ICU admissions to Swedish ICUs in 2017, those mechanically ventilated ≥ 7–21 d accounted for 1,643 (4%) admissions, and those with PMV > 21 d accounted for 307 (0.8%) admissions. Of the 109,457 ICU bed days, 22% were consumed by admissions ventilated ≥ 7–21 d and 10% by those with PMV > 21 d. The ICU mortality of both groups was 21%. Admissions with mechanical ventilation ≥ 7 d had a median age of 65 y and were predominantly male (64%).
CONCLUSIONS: Admissions to Swedish ICUs who required mechanical ventilation ≥ 7–21 d and PMV > 21 d form a relatively small proportion of all ICU admissions, but consume a significant proportion of ICU beds days. Prevalence of admissions, ICU bed days, and ICU mortality were lower than reports from other countries, but the admissions were predominantly elderly and male, in accordance with other reports.
Introduction
Mechanical ventilation in the ICU is a common and necessary treatment that allows patients to recover from the underlying causes of acute systemic or respiratory failure.1 Some patients have a prolonged requirement for mechanical ventilation due to the underlying disease or disorder or due to ventilatory weaning failure. The prevalence of patients requiring prolonged mechanical ventilation (PMV) is predicted to escalate, mainly due to an aging population with numerous comorbidities, placing additional burden on ICU services in the coming decades.2,3
Definitions of PMV range from ≥ 5 h to > 21 d in reported studies, despite a consensus conference in 2005 that defined PMV as mechanical ventilation > 21 d.4,5 Prevalence and characteristics of patients requiring PMV have been reported from the United States, Canada, China, the United Kingdom, and Brazil, with differing health care systems and with differing numbers of ICU beds.6-10 International studies from Canada and the United Kingdom have reported that the percentage of patients requiring PMV > 21 d constitute up to 4% of all ICU admissions and occupy 11–29% of available ICU bed days, resulting in a substantial impact on ICU resources.9,11 Furthermore, patients in need of PMV have higher mortality compared to other patients admitted to the ICU.7
Sweden has a publicly funded health care system, with consistent delivery of health care services throughout the country. The country is divided into 6 larger regions served by 7 tertiary care university hospitals responsible for all highly specialized care within each region and to which smaller hospitals within the region can transfer patients (https://skr.se/tjanster/englishpages.411.html, Accessed January 30, 2019).
Patients requiring PMV are treated in acute ICUs. Sweden does not have long-term acute care hospitals to receive patients after 21 d for weaning. Sweden has only 1 weaning center for patients experiencing PMV; this unit has 11 beds, is located in Stockholm, and is privately run but with agreements to accept patients from ICUs within the public health care system. Mechanical ventilation is not performed in wards outside the ICU with the exception of spinal cord injury wards, which train patients and caregivers on home ventilators before discharge. Compared to other European countries, Sweden has very few ICU/intermediate care beds, with only 5.8 beds/100,000 inhabitants (30th of 31 European countries).12
Data regarding intensive care are lacking from Sweden, a country that has almost no private health care providers within intensive care, and a small number of ICU beds in relation to the population. The primary aim of this study was to identify the prevalence of ICU admissions requiring mechanical ventilation ≥ 7–21 d and PMV > 21 d in Swedish ICUs, as well as the use of ICU bed days by these admissions. Secondary aims were to describe patient characteristics and patient outcomes (ie, mortaliy in ICU and at 30 d and 90 d), and to explore differences between baseline characteristics in admissions mechanically ventilated ≥ 7–21 d and with PMV > 21 d. The rationale to include admissions requiring mechanical ventilation ≥ 7 d was based on the timing of tracheostomy, proposed as a marker of PMV.13 In Swedish ICUs, tracheostomy is performed at ∼ 7.5 d after start of mechanical ventilation.14 Mechanical ventilation ≥ 7 d is also consistent with the transition to persistent critical illness, which generally occurs 7–10 d after ICU admission.15
Quick look
Current Knowledge
The number of patients on prolonged mechanical ventilation (PMV) is growing due to an aging population, and these patients consume a significant proportion of acute care and ICU resources. International studies on prevalence and resource utilization of this patient group exist, but data are lacking from a Scandinavian ICU population.
What This Paper Contributes to Our Knowledge
In this registry study conducted in Sweden, admissions to the ICU on PMV > 21 d constituted < 1% of all ICU admissions but consumed 10% of all ICU bed days. ICU mortality, prevalence, and use of ICU bed days was lower than in international studies. Limited access to ICU beds was not associated with increased ICU bed occupancy of subjects on PMV.
Methods
Study Design and Data Sources
We conducted a retrospective observational cohort study using data from the Swedish Intensive Care Registry (SIR) (http://www.icuregswe.org/en, Accessed November 18, 2018), a national ICU quality registry approved by the Swedish National Board of Health and Welfare (http://www.socialstyrelsen.se/english, Accessed November 14, 2018). The SIR contains prospectively collected data on all ICU admissions, recorded daily by members of the ICU team. The SIR commenced data collection in 2001; in 2017, 80 of the 84 (95%) Swedish ICUs were registry members and contributed data. This study was performed at the Institute of Health and Care Sciences, The Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden.
Admissions
Data from the SIR on all adult admissions (≥ 18 y old) to the ICU and receiving mechanical ventilation ≥ 7 d from January 2017 to December 2017 were requested. From these data, we created 2 subgroups, those ICU admissions ventilated ≥ 7–21 d and those requiring PMV > 21 d. We excluded data from pediatric ICUs and patients < 18 y old admitted to non-pediatric specialist ICUs. To obtain denominators to calculate prevalence, the percentage of ICU bed days used, and for mortality we used the SIR open-source data to identify all ICU admissions excluding data on patients < 18 y old. Registry data counts all admissions as a new episode of care, therefore patients re-admitted to ICU are counted as new admissions.
Variables
We requested from the SIR the following variables for each admission: age; sex; admission source (ie, ward/other ICU/emergency department/operating theater or recovery room/another hospital); condition at admission including co-morbidities, severity of illness assessed using the Simplified Acute Physiology Score version 3 (SAPS 3),16 and primary ICU diagnosis as documented using the International Classification of Diseases, Tenth Revision (ICD-10 SE); the day tracheostomy was performed; duration of mechanical ventilation; length of ICU stay; and mortality in the ICU and at 30 d and 90 d. We also identified the hospital type (university/non-university) for each admission.
SAPS 3 is based on ICU admissions data and was developed to assess the severity of illness to predict ICU outcomes. The SAPS 3 score is based on co-morbidities, reason for admission, and clinical data at admission.16 According to SIR (http://www.icuregswe.org/en, Accessed November 18, 2018), the ICD-10 SE is used in SIR to document the primary ICU diagnosis. Each ICU patient may meet criteria for several diagnoses but has only one “primary ICU diagnosis,” assigned by the most responsible physician before ICU discharge. Discontinuation of mechanical ventilation is defined as extubation without requirement for re-intubation within 24 h.
Ethics Approval
The study was approved by the Regional Ethical Review board in Gothenburg (no. 996–17) and was performed in adherence to the Declaration of Helsinki.17 After ethics approval, permission to receive requested data was obtained from SIR. All ICU patients or their next of kin are given a written standard document on ICU discharge informing them that data will be transferred to SIR and can be used for research after ethical approval. Patients or next of kin can opt out of their data being sent to SIR at this time.
Statistical Analyses
We used descriptive statistics to describe our cohort, using n (%) for categorical data and median (range) for continuous data. We performed logistic regression modeling to examine the association of sex, age, university/non-university ICU, SAPS 3 score, and diagnosis with the need for PMV > 21 d compared to admissions ventilated ≥ 7–21 d. We used SPSS 25.0 (IBM, Armonk, New York) and STATA 15.1 (StataCorp, College Station, Texas). All tests were 2-sided, and P values < .05 were considered significant.
Results
Unit Characteristics
We received data from 74 of 80 (93%) Swedish ICUs reporting to SIR. This excludes data from 4 pediatric ICUs; 2 other ICUs did not report data in 2017. Of the 74 ICUs, 22 (29%) were located in university hospitals; 13 of 22 (59%) were specialized ICUs (ie, neurology/neurosurgery, thoracic surgery, infection diseases, burns, and extracorporeal membrane oxygenation), and the remaining ICUs were located in non-university hospitals.
Patient Characteristics and PMV Prevalence
In 2017, there were 39,510 ICU admissions of patients ≥ 18 y old to the 74 ICUs submitting data to SIR; 1,643 of 39,510 (4%) ICU admissions required mechanical ventilation ≥ 7–21 d, and 307 of 39,510 (0.8%) required PMV > 21 d (Fig. 1). Demographic characteristics of all admissions requiring mechanical ventilation ≥ 7 d, including admissions ventilated ≥ 7–21 d, and admissions with PMV > 21 d are shown in Table 1. In 2017, 1,950 admissions with mechanical ventilation ≥ 7 d were admitted to Swedish ICUs. The median (range) age was 65 (18–89) y, with 1,103 of 1,950 (57%) being 61–80 y old and 113 of 1,950 (6%) being > 80 y old; 64% of all admissions were male admissions. Median (range) days from ICU admission to tracheostomy was 7 (0–45) d. The 2 most common primary ICU diagnoses were septic shock/severe sepsis and respiratory insufficiency. The 10 most common diagnoses are shown in Table 2.
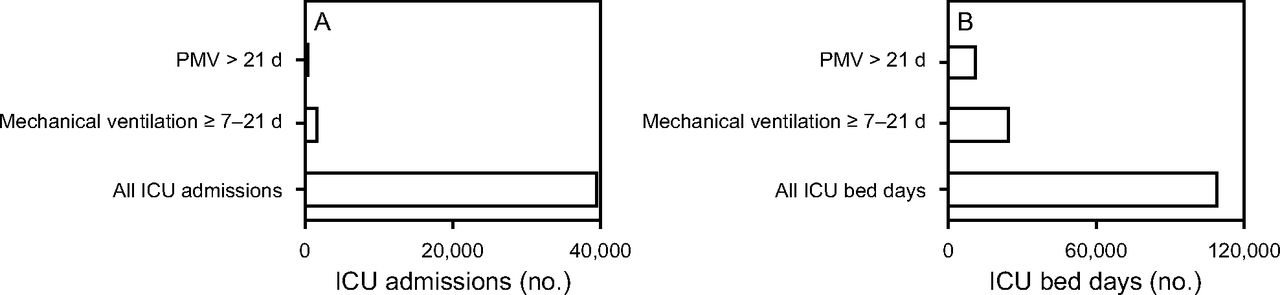
A: Prevalence of admissions with PMV > 21 d and mechanical ventilation ≥ 7–21 d in comparison to all ICU admissions in Swedish ICUs in 2017. B: Occupancy of ICU bed days for admissions with PMV > 21 d and mechanical ventilation ≥ 7–21 d in comparison to all ICU bed days in Swedish ICUs in 2017. PMV = prolonged mechanical ventilation.
Demographic Characteristics
The 10 Most Common Diagnoses
Use of Bed Days
Of the 15,564 admissions requiring mechanical ventilation, 1,643 (11%) required mechanical ventilation ≥ 7–21 d and 307 (2%) required PMV > 21 d (Fig. 1). The 39,510 admissions to the 74 Swedish ICUs reporting data to SIR in 2017 occupied 109,457 ICU bed days. The 1,643 admissions requiring mechanical ventilation ≥ 7–21 d occupied 24,250 ICU bed days, accounting for 22% of all ICU bed days. The 307 admissions with PMV > 21 d (10,985 of 109,457 bed days) accounted for 10% of all ICU bed days.
Mortality
ICU mortality was 9%, 30-d mortality was 18%, and 90-d mortality was 22% considering all 39,510 admissions in 2017 (Fig. 2). ICU mortality documented for the 1,643 admissions with mechanical ventilation ≥ 7–21 d was 21%, and the mortality for PMV > 21 d was the same. For admissions with mechanical ventilation ≥ 7–21 d, 30-d mortality was 32% and 90-d mortality was 40%, documented for 1,606 of 1,643 (98%) admissions. There was no difference in ICU or 90-d mortality for admissions ventilated ≥ 7–21 d and with PMV > 21 d. Admissions with PMV > 21 d had a lower 30-d mortality rate compared to admissions with mechanical ventilation ≥ 7–21 d (12% vs 32%, P < .001).

Mortality in subjects with mechanical ventilation ≥ 7–21 d and PMV > 21 d in comparison to all ICU admissions (with and without mechanical ventilation) in Swedish ICUs in 2017. All ICU admissions: n = 39,510 admissions; mechanical ventilation ≥ 7–21 d: n = 1606 admissions; PMV > 21 d: n = 301 admissions (missing data in admissions ≥ 7–21 and > 21 d: n = 43). PMV = prolonged mechanical ventilation.
Predictors for PMV > 21 d
There were no differences in sex, age, illness severity (SAPS 3 score), or hospital type for admissions requiring PMV > 21 d compared to those requiring mechanical ventilation ≥ 7–21 d. Admissions requiring PMV > 21 d were more likely to have a primary ICU diagnosis of pancreatitis (odds ratio 2.98, 95% CI 1.44–6.15) or respiratory insufficiency (odds ratio 1.65, 95% CI 1.08–2.52) compared to admissions requiring mechanical ventilation ≥ 7–21 d, adjusted for sex, age, university or non-university ICU, SAPS 3 score, and other diagnoses (Table 3).
Variables Associated With PMV > 21 d Compared to Mechanical Ventilation ≥ 7–21 d
Discussion
In this Swedish ICU registry study, the prevalence of admissions from 2017 who required mechanical ventilation ≥ 7–21 d made up 4% of all ICU admissions; those requiring PMV > 21 d comprised 0.8%. Admissions with mechanical ventilation ≥ 7–21 d accounted for 22% of all ICU bed days, whereas those with PMV > 21 d accounted for 10%. The ICU mortality in the 1,950 admissions with ventilated ≥ 7–21 d and PMV > 21 d was 21%, compared to 9% for all ICU admissions. Only a diagnosis of pancreatitis or respiratory insufficiency distinguished admissions requiring PMV > 21 d compared to mechanical ventilation ≥ 7–21 d.
The Swedish prevalence of PMV > 21 d (0.8%) is lower than that reported in studies from the United Kingdom and Brazil, which have noted a 4% prevalence accounting for all ICU admissions (ie, ventilated and non-ventilated).9,10 Also, the 2% prevalence of PMV > 21 d accounting for ICU admissions requiring mechanical ventilation only is somewhat lower than that reported in studies from the United Kingdom (6%), Brazil (10%), and Canada (5%).7,9,10 In our study, admissions requiring PMV > 21 d consumed 10% of all ICU bed days, which is more in accordance, although at the lower boundary of estimates, with international studies reporting that patients requiring PMV > 21 d use 11–29% of ICU bed days.9,11 This lower prevalence and low use of ICU bed days may be due to Sweden having one of the lowest number of ICU beds (ie, 5.8/100,000) of all European countries.12 However, data from this study indicate that, despite the low number of ICU beds available in Sweden, the percentage of ICU bed days occupied by admissions in need of PMV > 21 d was lower than in countries with access to more ICU beds.
In all 1,950 admissions ventilated ≥ 7 d, males accounted for 64% of all admissions, which is consistent with other studies, indicating that more male patients are treated in ICUs and they use more ICU resources.18,19 The median age of the 1,950 admissions was 65 y, and the age group 61–80 y was larger than all other age groups together, which is also in line with what has been reported in other studies.6,7 In our study, the 2 most common ICU diagnoses in admissions with mechanical ventilation ≥ 7–21 d and PMV > 21 d were septic shock/severe sepsis and respiratory insufficiency. Comparison of diagnosis profiles with other studies is difficult due to different methods of documenting a primary ICU diagnosis.7,9,18,19 However, earlier studies also reported sepsis as a primary reason of PMV.11,20 The only difference that we noted between admissions ventilated ≥ 7–21 d and those with PMV > 21 d was that a primary ICU diagnosis of pancreatitis or respiratory insufficiency was more likely to require PMV > 21 d.
ICU mortality in our study for admissions mechanically ventilated ≥ 7–21 d and PMV > 21 d was 21%, slightly lower than rates reported by other published studies in which ICU mortality ranged from 26% to 52%.9,10,21 The 30-d mortality rate was significantly lower in admissions with PMV > 21 d compared to those with mechanical ventilation ≥ 7–21 d (12% vs 32%). At first glance, this could be explained by a higher ICU mortality due to admissions requiring mechanical ventilation ≥ 7–21 d suffering from more severe conditions. This was not supported by data in our study, however, because severity of the clinical condition assessed by SAPS 3 did not differ between the groups. Another possible explanation for the lower 30-d mortality rate for admissions with PMV > 21 d compared to those with mechanical ventilation ≥ 7– 21 d could be decisions made on the futility of intensive care in the period between 7 and 21 d.
Surprisingly, at least during non-pandemic circumstances, a lower number of ICU beds did not increase the percentage of ICU bed occupancy by admissions requiring PMV. The lower prevalence of admissions requiring PMV in Sweden is likely multi-factorial and possibly due a healthier population, a differing prevalence of patients with greater severity of illness, differing admission or discharge criteria, or the availability of noninvasive ventilation in high-dependence wards. However, because respiratory insufficiency was one of the diagnoses that was significantly more common in the group of admissions who were in need of PMV > 21 d, the ongoing COVID-19 pandemic could certainly affect these results.
Difficulties in weaning from PMV have been described as a great challenge, with persistent or chronic critical illness gaining increasing interest in recent decades.22,23 To optimize care for patients with persistent time in ICU, care should be managed by fully integrated interdisciplinary teams including optimized strategies for the weaning process, including family-focused care.23-25 Sweden has a tradition of interdisciplinary teams working close together in the ICU, including physicians, nurses, and physiotherapists, all specialized in ICU care. Different weaning protocols are used in most ICUs, and there are no national guidelines. This could have influenced the results in this study.
To improve the weaning process further, a shift to more person-centered care could be worth studying, even though seeing the patient as a person with resources and able to be active in collaborative care could be a challenge in an ICU environment due to sedation, severity of illness, and communication difficulties.26 There is a lack of intervention studies of person-centered care in the ICU environment, although it has been reported to reduce length of hospital stay and costs in non-ICU settings.27,28
Limitations
This study has several limitations. First, our data covered only 1 y, and therefore we were unable to model PMV prevalence trends over time. Second, the registry does not hold data related to weaning duration or weaning failure, which may have helped explain the low prevalence rates in Swedish ICUs because PMV is frequently a sign of unsuccessful weaning. Finally, use of data from registries is dependent on correct reporting of data, and analyses are restricted by the data available in the registry.
Conclusions
In 2017, admissions to Swedish ICUs requiring mechanical ventilation ≥ 7–21 d and PMV > 21 d comprise a relatively small proportion of all ICU admissions but consume a significant part of ICU beds days. Despite a low number of ICU beds on a national level, Swedish admissions requiring PMV > 21 d was lower than reports from other countries. Also, ICU bed days and ICU mortality in admissions requiring PMV > 21 d were lower than most reports from other countries. However, according to international studies, a predominant part of admissions was older and mostly male. Further research is needed to explore strategies to optimize the use of limited ICU resources by reducing the duration of mechanical ventilation for patients requiring PMV.
Acknowledgments
The authors thank Max Petzold, Professor in Health Science Statistics, Department of Public Health and Community Medicine, Institute of Medicine, Sahlgrenska Academy, University of Gothenburg, Sweden for statistical support. The authors also thank the board of The Swedish Intensive Care Registry.
Footnotes
- Correspondence: Carl-Johan Cederwall MSc RN, Sahlgrenska University Hospital, CIVA, Gröna stråket 2, 413 45 Gothenburg, Sweden. E-mail: carl-johan.cederwall{at}vgregion.se
This work was supported in part study by grants from the Swedish state (ALFGBG-74160). The authors have disclosed no conflicts of interest.
- Copyright © 2021 by Daedalus Enterprises





{kind=link}
{kind=link}