

Abstract
BACKGROUND: Patients with neuromuscular disorders (NMD) share the risk of acute respiratory failure (ARF) leading to ICU admissions. Noninvasive ventilation (NIV) is often proposed as an alternative to invasive ventilation. This study describes clinical features, ventilation management, and outcomes of subjects with NMD admitted to ICU and managed for ARF.
METHODS: We performed a multicenter retrospective study in 7 adult ICUs in the Auvergne-Rhone-Alpes area in France involving subjects with NMD admitted to the ICU for ARF. The primary end point was ICU mortality. Secondary end points were NIV failure, weaning from invasive ventilation, and long-term mortality. We hypothesized a poorer outcome in the case of bulbar musculature involvement.
RESULTS: A total of 242 subjects were included; 142 subjects had nonhereditary NMD (58.7%), and 100 had hereditary NMD (41.3%). Eleven subjects had home ventilation through a tracheostomy. While 112 were intubated at admission, 119 initially underwent NIV. NIV was successful in avoiding orotracheal intubation in 78 subjects (65.5%). ICU mortality was 13.6%. Factors associated with ICU mortality were nonhereditary NMD and requirement for invasive ventilation. The involvement of bulbar musculature in ARF and hereditary NMD were associated with NIV failure. After a median follow-up of 1.2 y, 53 of 209 subjects had died.
CONCLUSIONS: The ICU mortality of NMD subjects with ARF was low, with no impact of bulbar muscles involvement. NIV was proposed for approximately half of the subjects, and it was more effective when ARF was not attributed to bulbar musculature involvement. The long-term outcome was good.
- acute respiratory failure
- noninvasive ventilation
- neuromuscular disorders
- ventilator weaning
- long-term prognosis
- mechanical ventilation
Introduction
Neuromuscular disorders (NMD) are a rare and heterogeneous condition. Though NMDs differ according to evolution and physiopathology, they share the risk of acute respiratory failure (ARF) in a chronic restrictive disorder that may eventually result in ICU admission. The problems concerning hereditary and nonhereditary NMDs are similar, but they differ in terms of clinical management: the main challenges are determining the right time to intubate a patient with nonhereditary NMD so as to avoid the risk of aspiration pneumonia, and, when noninvasive ventilation (NIV) management is preferred in patients with hereditary NMD, avoiding a situation that lead to difficult weaning from invasive ventilation.
NMD-related ARF is commonly thought to result from 3 mechanisms: hypoventilation due to inspiratory muscle involvement; inefficient cough due to expiratory or inspiratory muscle involvement; and upper airway obstruction and swallowing impairment due to bulbar muscle involvement.1,2 Muscular respiratory weakness leading to a restrictive respiratory pattern and hypoventilation are the main feature of ARF in patients with NMD, leading to hypercapnic respiratory failure.
Respiratory care for patients with NMD specifically includes cough assistance and ventilatory support. NIV is often proposed, whenever possible, as an alternative to invasive mechanical ventilation.3-5 Indeed, orotracheal intubation (OTI; includes nasotracheal intubation) is a crucial event as ventilation weaning is difficult in these patients and can lead to definitive tracheostomy. NIV failure can be attributed to the progression of NMD and various patterns of respiratory muscles impairment, most importantly diverse bulbar muscles dysfunctions.6,7
Very few studies have described the prognosis and ventilatory management of subjects with NMD.8,9 Hence, there are no guidelines for ICU management of patients with NMD.3,10,11 This study aimed to describe: (1) the clinical features of subjects with NMD presenting with ARF leading to ICU admission; (2) ventilatory management, NIV failure, and weaning from invasive ventilation during ICU stay; (3) ICU mortality and its determinants; and (4) long-term prognosis in ICU survivors. Such information is useful for clinicians to quickly identify subjects who are more likely to benefit from either invasive ventilation or NIV. We hypothesized that bulbar muscle involvement is associated with ICU mortality, NIV failure, weaning failure, and long-term mortality.
QUICK LOOK
Current knowledge
Few studies describe the prognosis and the ventilatory management of subjects with neuromuscular disorders (NMD) experiencing acute respiratory failure. Noninvasive ventilation (NIV) is often proposed, although data supporting its use in an acute setting are scarce. There is a lack of clarity around which characteristics make patients with NMD and acute respiratory failure more likely to benefit from NIV, and which characteristics make them more likely to be successfully weaned from invasive ventilation.
What this paper contributes to our knowledge
The short-term prognosis of subjects with NMD who presented with acute respiratory failure was good, but the mortality was higher when invasive ventilation was used. NIV had a high success rate when used in subjects with an acute respiratory failure that did not involve the bulbar musculature. Half the subjects with NMD who underwent orotracheal intubation were successfully weaned from mechanical ventilation.
Methods
This was a multicenter retrospective observational study. We reviewed the medical records of consecutive patients admitted to 7 medical ICUs in the 4 university hospitals in the Auvergne-Rhone-Alpes area in France for a first ICU stay between January 1, 2007, and December 31, 2015. These wards were medical ICUs or medico-surgical ICUs. One ICU was a regional referral respiratory care unit. Subjects were preselected according to medical information system program data.
Inclusion and Exclusion Criteria
Subjects were included if they met all the following criteria: age ≥ 18 y, first admission in ICU for ARF during the period considered (no duplicate), and history of NMD. ARF was defined as breathing frequency > 35 breaths/min, signs of respiratory distress were present, uncompensated hypercapnia was present, or the subject needed any increased oxygen or ventilatory support. The NMD considered were Duchenne muscular dystrophy, Steinert myotonic dystrophy, other hereditary neuropathy or myopathy, inflammatory myopathy, amyotrophic lateral sclerosis, myasthenia gravis, Guillain-Barré syndrome, post-traumatic tetraplegia, or other acquired neurologic disorder. A pediatrician, neurologist, or internist validated the diagnosis. Any of the following criteria was a reason to exclude the subject: non-formerly diagnosed NMD, prior ICU-acquired weakness, ICU stay for other reasons than ARF, and perioperative setting.
Data Collection
Data were retrospectively collected from subjects’ medical charts. At the time of ICU admission, we collected data related to the previous condition: demographics, NMD and ventilatory characteristics, Charlson comorbidity Index,12 Sequential Organ Failure Assessment (SOFA)13 items, arterial blood gases, Simplified Acute Physiology Score (SAPS) II,14 presence of upper or lower respiratory tract infection, and neuromuscular mechanism(s) leading to ARF (eg, inspiratory muscles involvement was considered when hypoventilation or ultrasonography diaphragmatic dysfunction was present; cough impairment was considered when airway secretions clearance or cough failure were mentioned; bulbar muscle involvement during phonation, or swallowing disorders or aspiration pneumonia were present).
We collected the following data from the subjects’ ICU stay: ARDS with  < 150 mm Hg,15 sepsis,16 complications of tracheal tube, need for fiberoptic aspiration, NIV failure (defined as death or OTI), type and duration of ventilatory support, weaning characteristics (eg, number of spontaneous breathing trials and extubations, duration of weaning), placement of tracheostomy, and end-of-life decision or advanced directive. We also collected vital and ventilatory status at the time of ICU discharge, as well as data on the long-term outcomes (ie, survival after ICU discharge, ICU readmission, and tracheostomy during follow-up).
< 150 mm Hg,15 sepsis,16 complications of tracheal tube, need for fiberoptic aspiration, NIV failure (defined as death or OTI), type and duration of ventilatory support, weaning characteristics (eg, number of spontaneous breathing trials and extubations, duration of weaning), placement of tracheostomy, and end-of-life decision or advanced directive. We also collected vital and ventilatory status at the time of ICU discharge, as well as data on the long-term outcomes (ie, survival after ICU discharge, ICU readmission, and tracheostomy during follow-up).
Statistical Analysis
Follow-up was completed until December 31, 2017. The primary end point was ICU mortality. Secondary end points were NIV failure in subjects initially treated by NIV, success of weaning from invasive ventilation in subjects undergoing OTI, and long-term survival after ICU in ICU survivors. To reduce bias due to missing data, we conducted a multivariable imputation by chained equations (MICE) procedure for incomplete variables (marked *) and the random Forrest method with 15 iterations and a single dataset. The seed was set to 2,690. The plausibility of the imputed values was checked by comparing the distribution of the variables before and after imputation and by examining density plots.
Data were expressed as mean ± SD for quantitative variables, and count (percentage) for qualitative variables. Normality distribution hypothesis was verified with the Kolmogorov-Smirnov test and graphically. Qualitative variables were compared using the chi-square test or Fisher exact test. Quantitative variables were compared using the Student t test or the Wilcoxon test. Univariable analysis was conducted using logistic regression. To identify risk factors independently associated with outcome, significant variables in the univariable comparison between survivors and nonsurvivors, between NIV success and failure, or between ventilation weaning success and failure (threshold 0.2) were entered into a multivariable backward stepwise logistic regression analysis, including the respiratory specialization of ICU centers. Kaplan-Meier graphs were drawn for long-term survival and compared using the Log Rank test. Long-term prognostic factors were assessed using a semi-parametric Cox model after verification of risk-proportionality hypothesis. Results are presented as odds ratio (OR) and their 95% CIs. The statistical significance threshold was set at P < .05. The analysis was performed using STATA 12 (StataCorp, College Station, Texas) and the CBCgrps17 and MICE libraries18 of the R software (R Foundation for Statistical Computing, Vienna, Austria).
Ethical Considerations
The study was approved by an ethics committee (CPP Sud-Est IV, agreement 16–124). Data collection was approved by the Health Information Processing Advisory Committee (CCTIRS 17-065). Subjects’ informed consent was waived according to French legislation.
Results
Description of the Cohort
A total of 242 subjects were included. Subjects’ characteristics at baseline are described in Table 1. Mean age was 55 ± 20 y, and 146 subjects were male (60.3%). NMD were clustered into 2 groups: 142 had nonhereditary NMD (58.6%), and 100 had hereditary NMD (41.3%). Fifty-seven subjects (23.6%) had chronic NIV before ICU admission. Eleven subjects (4.5%) had long-term home ventilation through a tracheostomy. In addition to ARF, 70 subjects (28.9%) presented with one or more concurrent organ failure. Respiratory tract infection was present at admission in 181 subjects (74.8%); 109 subjects had hypercapnia (49.3%), 112 were nonhypercapnic at ICU admission. Blood gas analysis was missing in 21 subjects The characteristics of hypercapnic and nonhypercapnic subjects are provided in the online supplement (see the supplementary materials at http://www.rcjournal.com).
Baseline Characteristics
Management During ICU Stay
ICU stay was complicated with the occurrence of new organ failure in 112 cases (46.2%) (see the supplementary materials at http://www.rcjournal.com). Of the 231 tracheostomy-naive subjects, 112 were intubated on the first day. Among the remaining 119 subjects who underwent NIV initially, 41 eventually received OTI or died. NIV was successful in avoiding OTI in 78 subjects (65.5%). Of the 151 subjects who had OTI, 19 had local complications related to the tracheal tube (12.6%). Of the 151 subjects who had OTI in the ICU, 116 underwent a weaning strategy (76.8%), 19 subjects died before weaning was considered (12.6%), and 16 were directly headed to tracheostomy despite no contra-indication to weaning (10.6%) (Fig. 1). NIV was successfully initiated in the ICU in 48 subjects. The flow charts of hereditary and nonhereditary NMD subjects are shown in the online supplement (see the supplementary materials at http://www.rcjournal.com).

Flow chart. NMD = neuromuscular disease, PMV = prolonged mechanical ventilation, NIV = noninvasive ventilation.
Outcomes
ICU Mortality.
The median ICU length of stay was 10 d. Thirty-three subjects died in the ICU (13.6%). The main cause of death was respiratory in 20 cases (60.6%), and nonrespiratory causes constituted 13 cases (39.4%). Table 2 compares ICU survivors and nonsurvivors among the 242 subjects and shows the results of univariable analysis. Long-term ventilatory support before ICU admission was not different between survivors and nonsurvivors. Compared to subjects who survived, SAPS II was higher (P = .001) and concurrent nonrespiratory failure at admission was more frequent (P = .003) in subjects who died in the ICU. The attributed neuromuscular mechanisms of ARF were not significantly associated with survival. Respiratory tract infection at ICU admission was associated with survival (P = .005). Results of blood gas analysis at ICU admission did not differ between survivors and nonsurvivors. Invasive ventilation was associated with poorer outcomes (P = .005). SAPS II, existence of nonhereditary NMD (compared to hereditary NMD), requirement for invasive ventilation, and ARDS with  < 150 mm Hg were covariates independently associated with ICU mortality, whereas respiratory tract infection at ICU admission was an independent protective marker (Table 3).
< 150 mm Hg were covariates independently associated with ICU mortality, whereas respiratory tract infection at ICU admission was an independent protective marker (Table 3).
Univariable Analysis of Mortality at ICU Discharge
Multivariable Analysis of Mortality at ICU Discharge
NIV Failure.
Of the 119 subjects who underwent initial NIV, subjects with hereditary NMD were more likely to undergo NIV failure (P = .007) (see the supplementary materials at http://www.rcjournal.com). Subjects on previous long-term NIV succeeded with NIV as the initial strategy more often than subjects with no history of ventilatory support (P = .006). Previously identified bulbar musculature impairment (P = .29) was not significantly associated with NIV failure, but attribution of ARF to bulbar muscle involvement was (P = .001). Involvement of bulbar musculature in ARF, acidosis at ICU admission, and existence of hereditary NMD (compared to nonhereditary NMD), but not a previous NIV support, were independent markers of NIV failure after adjusting for confounders (see the supplementary materials at http://www.rcjournal.com).
Weaning From Invasive Ventilation.
For the 116 subjects who underwent a ventilation weaning process, 76 were definitively extubated and discharged alive (65.5%). Median duration of invasive ventilation before the first separation attempt from ventilator was 5 d. Subjects with nonhereditary NMD were more likely to be successfully weaned from invasive ventilation than subjects with hereditary NMD (see the supplementary materials at http://www.rcjournal.com). Ventilatory condition prior to ICU stay did not show a significant role in weaning outcome. The same was true for previously identified bulbar muscles impairment, SAPS II, and neuromuscular mechanism of ARF. Hospitalization in the specialized respiratory ICU was associated with success of weaning compared to nonspecialized centers. Subjects who refused tracheostomy in cases of weaning failure showed a weaning success rate similar to that for subjects who did not refuse it. The probability of successful weaning from invasive ventilation decreased as the number of extubations increased. Age, nonhereditary NMD, and short duration of invasive ventilation were independently associated with weaning success, while the ICU center was not a risk factor for weaning outcome in multivariable analysis (see the supplementary materials at http://www.rcjournal.com).
Follow-up after ICU Discharge.
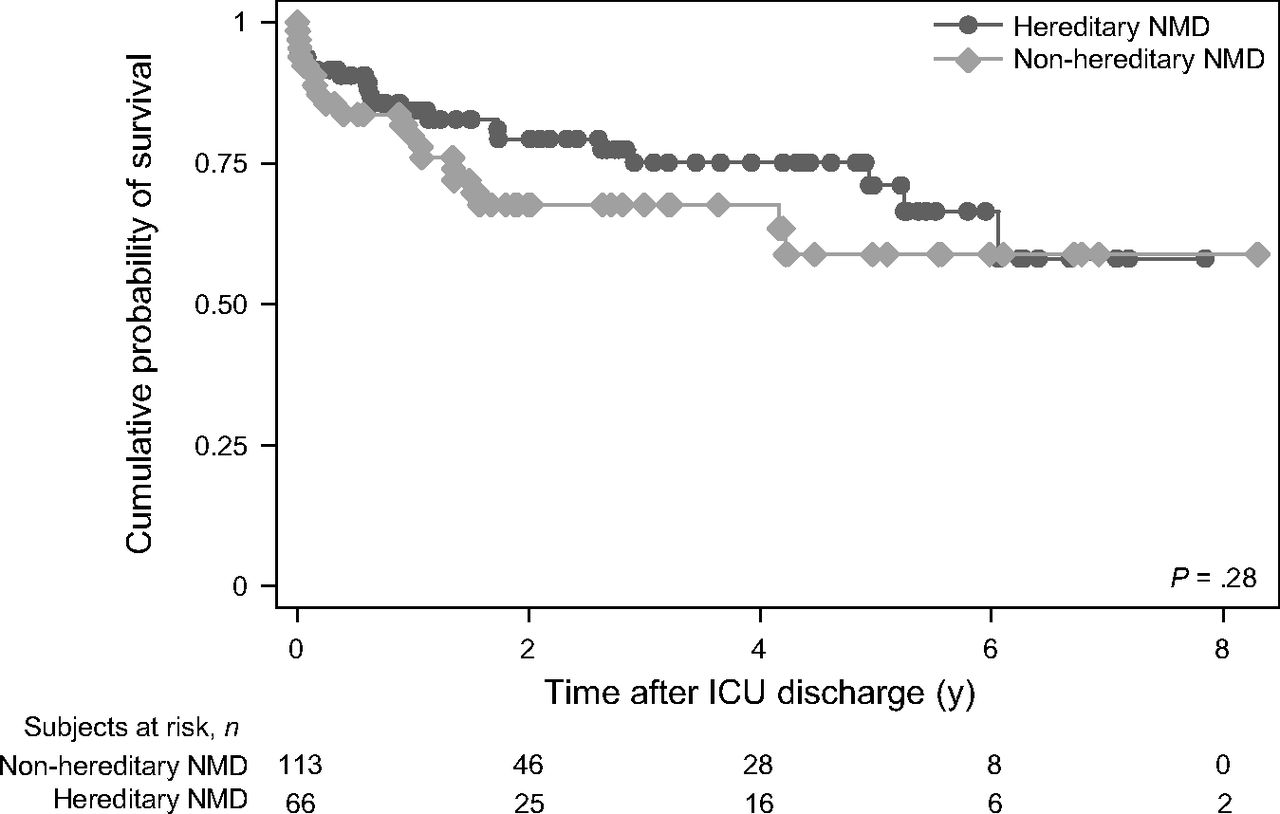
Long-term information was available in 179 subjects. Median follow-up after ICU discharge was 1.2 y; 1-y survival was 81% (95% CI 73–85), and 5-y survival was 61% [50%–69%]. Figure 2 displays hereditary and nonhereditary NMD survival curves after ICU discharge. Fifty-seven subjects were readmitted to the ICU with a median duration between ICU discharge and first ICU readmission of 4 months. Ten subjects underwent tracheostomy, and 20 subjects refused it. During follow-up, 53 subjects died. The main cause of death was respiratory in 28 cases (53%), extrarespiratory in 18 (29%), and unknown in 7 cases (18%).

Kaplan-Meier graph of cumulative survival probability after ICU discharge in subjects with hereditary and nonhereditary neuromuscular disease (NMD).
Age, comorbidities, and advanced directive influenced long-term mortality (see the supplementary materials at http://www.rcjournal.com), whereas the subtype of NMD showed no influence. Inspiratory muscle involvement in initial ARF was associated with poorer long-term outcome, while other mechanisms had no impact. Multivariable analysis revealed that only age (P = .01) and Charlson comorbidity index (P = .032) were associated with a worse long-term outcome.
Discussion
The main findings of our study, in one of the largest reported cohorts of NMD subjects managed in the ICU for ARF and with long-term follow-up data, were: (1) ICU mortality was rather low (13.6%); (2) overall NIV exhibited a high success rate (65.5%), which was lessened with bulbar muscle involvement in ARF; (3) successful extubation occurred in 50.3% subjects undergoing OTI and invasive ventilation in ICU, mostly in subjects with nonhereditary NMD; and (4) the long-term outcome in survivors of ICU stay was good and was not dependent on either hereditary or nonhereditary NMD.
Short-Term Prognosis During ICU Stay
The ICU mortality of subjects with NMD was low as previously reported (< 10% for Guillain-Barré syndrome and myasthenia gravis,19-21 20% for amyotrophic lateral sclerosis22). In our study, diagnosis of respiratory tract infection at ICU admission was significantly associated with better survival. This finding may reflect that respiratory tract infection is a reversible cause for ARF, contrary to other causes that might reflect irreversible evolution of the underlying NMD. Invasive ventilation was associated with a poor outcome as previously reported,23,24 emphasizing the need to make every effort to avoid OTI in this specific population, and hence to optimize NIV management.
NIV Management
There is little evidence to support the use of NIV in this setting,23,24 yet NIV was applied in more than half of our subjects. NIV was previously reported to be effective in avoiding OTI in 79% of subjects with NMD,24 which is consistent with our findings (65.5%). Previous studies have suggested some physiological measures as predictors of OTI need, such as low tidal volume,25 vital capacity, and maximum pressures. Some of these measurements are difficult to record accurately in a retrospective study. Acidosis at ICU admission was associated with NIV failure, which corroborates previous results regarding hypercapnia.26
Swallowing disorders may compromise the effectiveness of NIV.27 However, our results indicate that previously identified bulbar muscles disorders were not as predictive of NIV failure as was bulbar musculature weakness leading to ARF, which emphasizes the need for accurate mechanistic diagnosis at ICU admission. Clinicians should not deny NIV solely on the existence of bulbar muscle impairment if such deficiency is not clearly involved in the etiology of ARF. We could not retrospectively assess the severity of such swallowing disorders, which might be a parameter to review. The nosologic framework of the NMD might influence the way bulbar muscle weakness is considered a warning for careful evaluation of need for OTI.28,29 We noted that subjects under previous long-term NIV had a similar NIV outcome in critical settings compared to those without previous NIV use: they both should benefit from NIV. A limitation to such a conclusion is that patients undergoing long-term NIV are more likely to be hospitalized in the ICU than NIV-naive subjects, even though their respiratory problem is milder, because NIV has to be managed by trained teams, mostly ICU teams. Even though NIV should be used with caution in patients with NMD and ARF, we observed that 48 subjects clearly benefited from successful NIV introduction in the critical setting.
Weaning from Invasive Ventilation
Subjects with NMD often belong to the subgroup “prolonged weaning,”30 or group 3 following the WIND classification (no successful weaning 7 d after the first attempt).31 Nonetheless, they represent < 10% of this subgroup in general settings.31,32 Consistent with the WIND study, among subjects undergoing OTI, 23.2% belonged to the group “no weaning process.” Nevertheless, mortality in this group was lower than in the corresponding group in the WIND study (54% vs 86%).31 This may reflect a limitation either of our retrospective data collection or of the a priori assumption of the clinicians about the weanability of subjects with NMD.
Subjects with NMD who had unsuccessful weaning represented 20.5%, which is much higher than the 3% rate reported in general settings.31 It has been proposed that some physiological measures may predict extubation success, such as transdiaphragmatic pressure variation.33 In actual practice, these parameters cannot be measured easily. Bach described the efficient management of subjects with “unweanable” NMD who could be extubated with intensive NIV and cough assistance after extubation.4 Respiratory physiotherapy, including cough augmentation techniques, plays a key role in preventing extubation failure and possibly protects against mortality.34-38 The data on respiratory physiotherapy were unavailable in the retrospectively reviewed medical charts. This was a major limitation of our study.
A protocolized systematic approach has proved its efficiency to reduce the length of invasive ventilation in general ICU populations,39,40 but this question remains unresolved for patients with NMD. There is no guideline concerning which strategy should be applied and for how long. Patients with a low vital capacity are highly susceptible to failing a spontaneous breathing trial, but some can be extubated.4,5 We found no independent association between number of extubations and weaning success. This reinforces the fact that, like in other subgroups of intubated subjects, attempts to provide intubated patients with NMD with a separation attempt should be done even though previous attempts had failed.
Although the literature describes the prognostic contribution of swallowing disorders to ventilation weaning,24,37 we found no association between bulbar muscle involvement and weaning failure. This could be explained by the fact that subjects with swallowing disorders might have been systematically been given tracheostomy without trying a weaning strategy.
Subjects with nonhereditary NMD were successfully weaned more often compared to those with hereditary NMD. This can traduce the often partially reversible neuromuscular mechanism for ARF in nonhereditary NMD.
Weaning centers have proven their efficiency in weaning subjects from invasive ventilation.41-44 In our study, hospitalization in the specialized respiratory ICU was not independently associated with the weaning outcome. This can be explained by the fact that, as a reference center, this weaning center regularly hosts subjects who already failed the weaning process in a previous nonspecialized ICU. Common critical illness severity scores rarely identified the unweanable subjects.42,45
Long-Term Prognosis
In a previous single-center study,46 we reported a 3-y survival rate of 58%. In this study, the survival rate 1-y after ICU discharge was 81%, confirming the finding of a good long-term outcome for subjects with NMD after ICU discharge. Such a finding should give confidence to intensivists while admitting subjects with NMD and ARF to the ICU. In non-ICU settings, the 5-y survival rate in subjects with NMD treated with NIV was 81%.47 Laub and Midgren48 reported that one of the determinants of long-term mortality was the initiation of mechanical ventilation in an acute setting.
Limitations and Strengths
Our study has several limitations. First, its retrospective design may have induced an information bias, and the data may not be detailed enough as discussed above. Some clinical signs of ARF that are specific to subjects with NMD could not be monitored, such as orthopnea. In the same way, detailed information on swallowing disorders and their severity was limited, and some useful physiological measures were not accessible in the retrospective data collection. In particular, it was not possible to measure the dose of NIV and the presence, intensity, and nature of manual or instrumental cough assistance; the low quality of data related to cough assistance, though essential, did not allow us to display it without major reservations. Second, our study was exploratory, so the numerous comparisons might have produced some artificial positive results. Third, we had no control group, either of normal subjects or of other respiratory diseases to compare with our observations. Finally, the long-term quality of life was not assessed and would deserve a prospective ad hoc follow-up investigation.
Our study had several strengths to note. The multicenter design improved the generalizability of our results. Our findings fill some knowledge gaps with regard to NMD and ARF. Our results should give confidence to internists and intensivists to avoid assigning a priori a poor prognosis in patients with NMD when they need ICU care. Our results might help guide clinicians in the decision-making process of difficult clinical situations. Finally, our study provides important long-term information, which is often lacking in the literature.
Conclusions
The ICU mortality of subjects with NMD and ARF was low and uninfluenced by bulbar muscle involvement. NIV performed in half the cases showed a high rate of success, and the rate lowered when bulbar musculature contributed to ARF. Successful extubation occurred in half of the subjects undergoing OTI. The long-term outcome in survivors of the ICU stay was good.
Footnotes
- Correspondence: Paul Chabert MD, Service de Médecine Intensive – Réanimation, Hôpital de la Croix Rousse, Hospices Civils de Lyon, 104, Grande rue de la Croix Rousse, 69004 Lyon, France. E-mail: paul.chabert{at}chu-lyon.fr
Supplementary material related to this paper is available at http://www.rcjournal.com.
The authors have disclosed no conflict of interest.
- Copyright © 2021 by Daedalus Enterprises





{kind=link}
{kind=link}