

Abstract
BACKGROUND: The perceptions of using noninvasive ventilation (NIV) during exercise in patients with COPD who are naïve to NIV is unknown. The present study aimed to examine the perceptions of using NIV during exercise in people with COPD and to determine the relationship between patient perceptions with both baseline patient characteristics and exercise outcomes.
METHODS: During a trial examining the effect of NIV during exercise on dynamic hyperinflation in people with COPD who were naïve to NIV, participants completed a 5-point Likert scale questionnaire (scored strongly disagree −2 to strongly agree +2) before and after using NIV during exercise and a semi-structured interview after using NIV during exercise.
RESULTS: Eighteen participants, mean age (SD) 69 (7) y, FEV1/FVC 0.44 (0.08), FEV1 39 (7)% predicted, completed the study. Prior to exercise with NIV, participants were neutral about NIV, (mean [SD]) (0.67[0.84]). After exercise with NIV, participants felt that NIV made breathing easier (1.00 [0.77]) and that it helped exercise (1.06 [0.64]). There were moderate correlations between feeling that NIV was comfortable or effective and a change in exercise endurance time (ρ = − 0.588, P = .02), isotime inspiratory capacity (ρ = 0.488, P = .03), and measures of resting hyperinflation (ρ = 0.603, \P = .02). Interviews revealed that despite feeling comfortable using NIV during exercise, NIV might be too complicated for patients to manage outside a supervised environment.
CONCLUSIONS: Individuals with COPD, naïve to NIV, and using NIV during exercise for the first time reported a positive effect of NIV on breathlessness and exercise performance. Participants’ perceived benefit of NIV correlated moderately with increased endurance time and resting hyperinflation and with a reduction in dynamic hyperinflation during exercise, suggesting that patient reports could also aid selection of those who will benefit from NIV during exercise.
Introduction
Pulmonary rehabilitation, with a key component of exercise training, is recommended in national guidelines as best-practice management for people with COPD.1-3 Noninvasive ventilation (NIV) as an adjunct to exercise in individuals with severe COPD can reduce exertional dyspnea and improve exercise capacity during a single exercise session.4-6 The use of NIV during exercise training over multiple sessions allows individuals to train at a higher intensity and achieve greater physiological training effects compared to exercise without NIV.7 However, individual responses to using NIV during exercise vary,5 and the effect of NIV during exercise training on exercise capacity after training is unclear, with health-related quality of life appearing no better or worse.7 While the routine use of NIV during exercise training is not recommended, NIV during exercise may have a role in assisting selected individuals who have a suboptimal response to exercise training.8 Despite the purported benefits of NIV, for people naïve to NIV, learning to breathe with NIV during exercise may be difficult and could be a source of variability in study findings.
Tolerance and acceptance of NIV during exercise may be linked to prior NIV experience. One study involving 50 participants with chronic hypercapnic respiratory failure secondary to severe COPD or severe restrictive thoracic disease, who were on long-term nocturnal NIV, found only one participant (4%) discontinued exercise training due to intolerance of NIV during exercise.9 In contrast, another study that recruited 33 participants with moderate COPD who were naïve to NIV reported that 5 participants (28%) were unable to tolerate NIV during exercise and withdrew from the study.10 Patient perceptions toward using NIV during exercise, especially in patients who are naïve to NIV, may impact both the tolerance and the efficacy of NIV during exercise. To date, perceptions about using NIV during exercise in people with COPD have not been studied. Further, it is unclear whether there is a relationship between patient perceptions of NIV during exercise and their baseline characteristics or exercise outcomes.
The present study aimed to (1) explore the perceptions of using NIV during exercise in patients with severe COPD who were naïve to NIV, (2) evaluate the relationships between individual perceptions of NIV during exercise and both baseline characteristics and exercise outcomes with NIV during exercise, and (3) identify potential barriers and facilitators to using NIV during exercise.
QUICK LOOK
Current Knowledge
The use of noninvasive ventilation (NIV) during exercise allows individuals to train at a higher intensity and achieve greater physiological effects compared to exercise without NIV. However, there is variability in the tolerance to NIV during exercise. Patient perceptions toward using NIV, especially in patients who are naïve to NIV, may impact both the tolerance and the efficacy of NIV during exercise.
What This Paper Contributes to Our Knowledge
Individuals with severe COPD who were using NIV during exercise for the first time perceived NIV as being effective at reducing breathlessness during exercise and increasing exercise endurance. Participants who perceived an improvement were more likely to have an actual change in exercise duration with NIV during exercise compared to exercise without NIV.
Methods
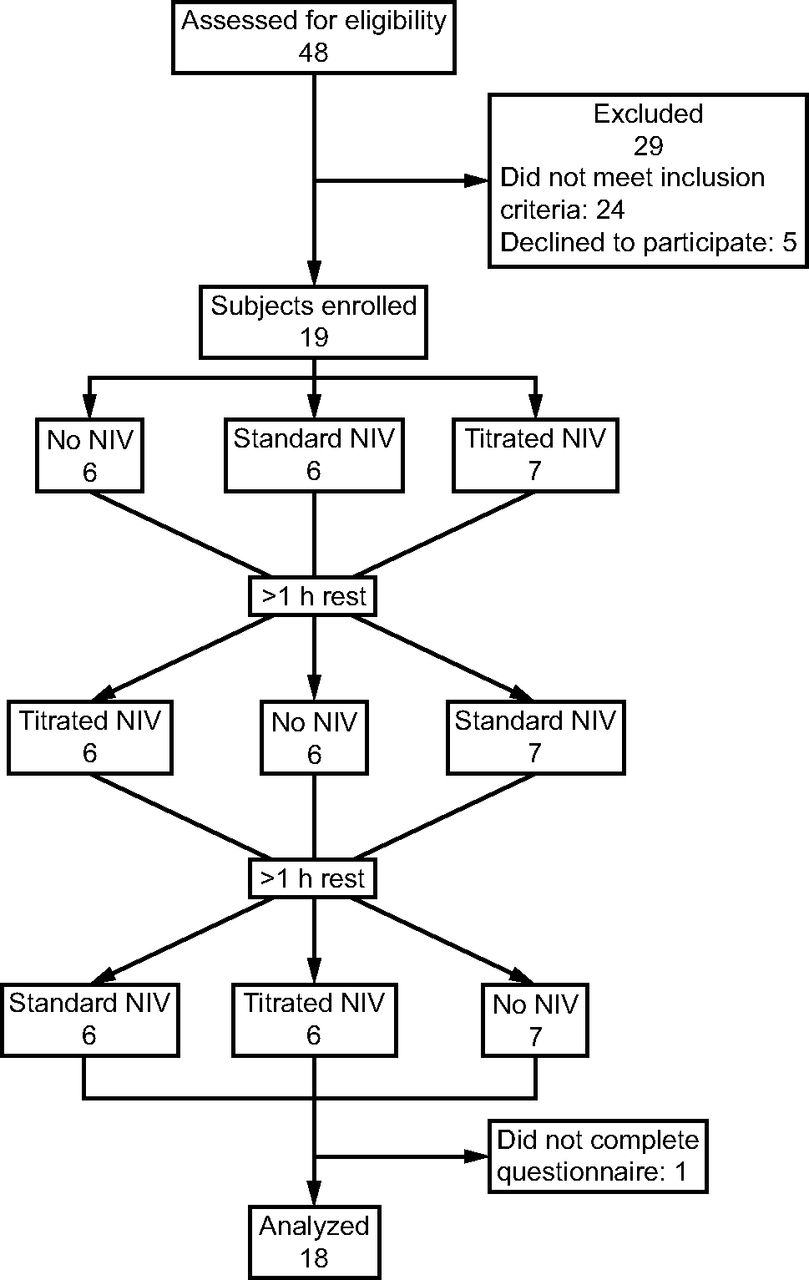
Participants were recruited as part of a randomized crossover trial examining the effects of NIV during exercise on dynamic hyperinflation and cycle endurance time in people with severe COPD attending pulmonary rehabilitation in Australia (Royal Prince Alfred Hospital, Sydney) and Germany (Schoen Klinik, Berchtesgadener Land), (Fig. 1, Ethics approval: HREC/13/RPAH/388 and 192/17; Trial registration: ACTRN12613000804785).11 Inclusion criteria were a diagnosis of COPD with an FEV1/FVC < 0.7, FEV1 < 50% predicted, a residual volume (RV)/total lung capacity (TLC) > 110% predicted, no exacerbations in the past 4 weeks, and dynamic hyperinflation classified as > 110 mL or > 11% reduction in inspiratory capacity (IC) during a peak incremental cycle test.12 Individuals were excluded if they had significant non-COPD lung disease, body mass index > 35 kg/m2, or nonrespiratory conditions that were likely to limit exercise performance.

Flow chart. NIV= noninvasive ventilation.
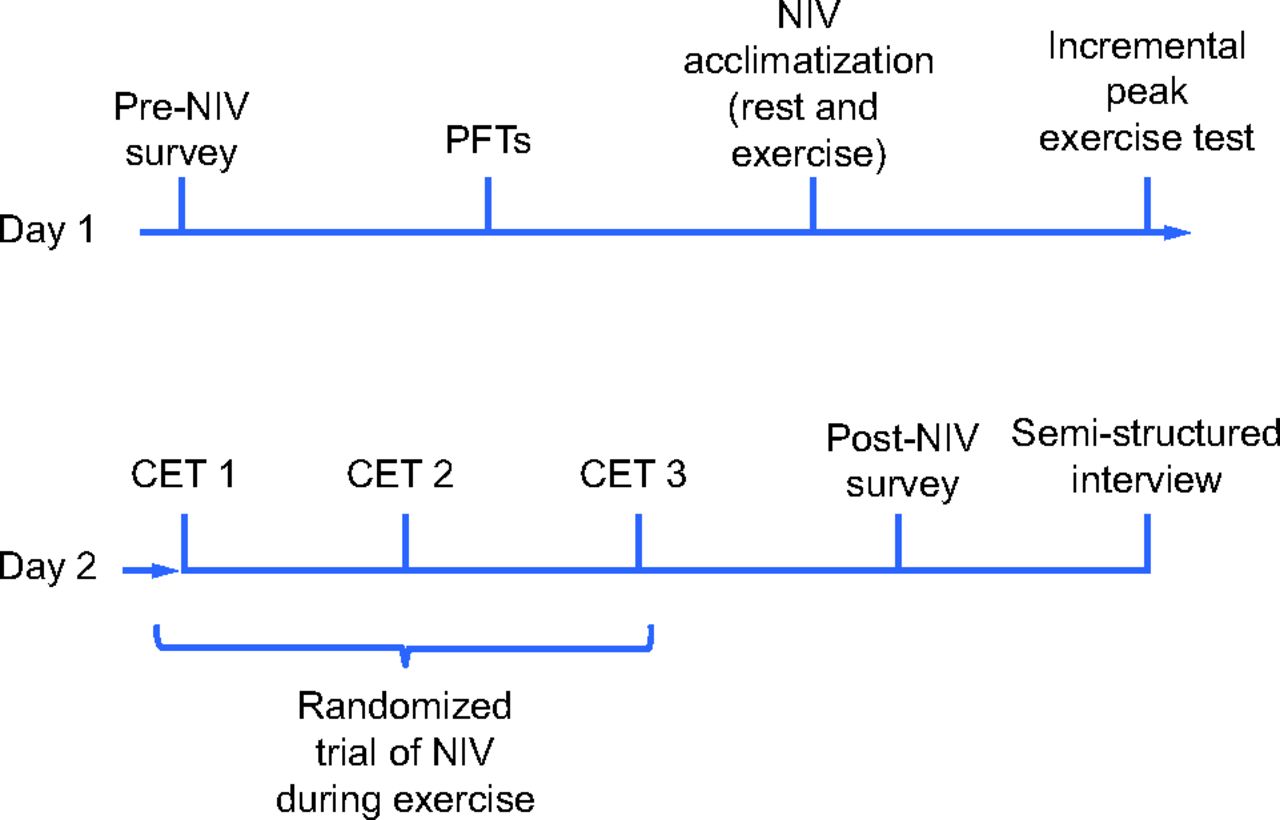
Methods for the randomized crossover trial have previously been reported.11 Briefly, pulmonary function tests, an incremental cycle test, and a short trial of NIV at rest and during exercise were performed on day 1. On day 2, participants performed 3 cycle endurance tests (CETs) to voluntary cessation (Fig. 2). The work rate was set at 75% of the peak work rate achieved in the incremental test. The 3 CETs were performed in random order: without NIV, with bi-level NIV using a standard expiratory positive airway pressure of 5 cm H2O, and with bi-level NIV using an individually titrated EPAP of 4.0 ± 1.2 cm H2O. The titrated EPAP was determined by trialing CPAP in 1-cm H2O increments from 4–8 cm H2O at rest. The level of pressure that maximized IC was selected.13 Pressure support of 11.0 ± 2.2 cm H2O was provided above EPAP. Bi-level NIV was delivered using an Astral 150 ventilator (ResMed, Sydney, New South Wales, Australia) with a dual-limb circuit and a full-face mask. Physiological variables were measured throughout exercise and compared between tests at isotime (the duration of the shortest test) and at end exercise.

Trial data collection time points. Survey questions and interview as well as baseline characteristics and exercise outcomes for correlation are shown. PFTs = pulmonary function tests; CET = cycle endurance test.
In the present study, participants completed 2 surveys (one on day 1 and one after the CETs on day 2) and a semi-structured interview after the CETs on day 2 (Fig. 2). The first survey (pre-NIV survey), performed at the beginning of day 1 of testing, included 6 questions about participants’ previous experience and perceptions of using adjuncts to manage their lung disease, such as supplemental O2, CPAP, or NIV. In addition, on a 5-point Likert scale, participants were asked to score whether breathlessness limited their exercise performance and if they would consider using an adjunct to manage breathlessness during exercise. Participants were also asked to nominate their preference of using either no adjuncts during exercise, supplemental O2, or NIV during exercise. Finally, participants were asked to describe the sensation of their exertional dyspnea by selecting one or more common descriptors of breathlessness.14
The second survey (post-NIV survey) was completed immediately following the last exercise session on the second day of testing, which was after using NIV during 2 exercise tests. Questions from the pre-NIV survey about participants’ perceptions toward the use of adjuncts to assist breathing during exercise were repeated. In addition, participants were questioned about the use of NIV during exercise after having had some experience. Using 5-point Likert scales, participants were asked a series of questions to determine if NIV during exercise was helpful, comfortable, and if they would consider using NIV during exercise in the future.
After completion of the post-NIV survey, a semi-structured interview was conducted with each participant. The investigator documented participants’ responses to each question and verified the accuracy of the documented responses with each participant. Questions were developed around 4 main issues associated with using NIV during exercise: comfort, ease of use, practicality, and feeling of benefit.
Analysis
Responses to the 5-point Likert scale questions from the pre-NIV and post-NIV surveys were converted into numerical data (strongly agree = 2, agree = 1, neutral = 0, disagree = −1, strongly disagree = −2) to allow the calculation of mean ± standard deviation (SD) and correlation with other variables. The relationships between post-NIV survey responses regarding the use of NIV during exercise and the change in cycle endurance time with NIV compared to exercise without NIV, as well as the difference in the change in IC from baseline to isotime exercise with NIV compared to exercise without NIV, were assessed by calculating Spearman rank correlation coefficients. The relationship between post-NIV survey responses regarding the use of NIV during exercise and both RV/TLC % predicted and change in IC during the incremental peak cycle test were also determined by calculating Spearman rank correlation coefficients. The interview questions guided the categories under which interview responses were coded. Three investigators individually read the responses and then agreed upon a set of codes for content analysis15 and reporting.
Results
Nineteen participants were recruited, and 18 completed the study (Table 1). No participants had previously used NIV. Two participants had previously used nocturnal CPAP, and 2 participants had experience using supplemental O2 via nasal prongs during a hospital admission.
Participant Characteristics
Pre-NIV survey responses are displayed in Figure 3. Most participants stated that breathlessness limited their ability to exercise. Participants’ preferences regarding the use of supplemental O2 via nasal cannula or the use of NIV via a mask during exercise were on average neutral (mean ± SD: 0.1 ± 0.7, 0.3 ± 0.7, respectively). However, there was a slightly higher preference for using supplemental O2 to assist breathing compared with NIV. The most common descriptor of breathlessness was “My breathing requires effort” (n = 8); however, all descriptors were given by at least one participant (Table 2).

Pre-NIV survey responses. Mean and SD calculated from scored responses. Responses scored as: strongly agree = 2; agree = 1; neutral = 0; disagree = −1; strongly disagree = −2.
Breathlessness Descriptors
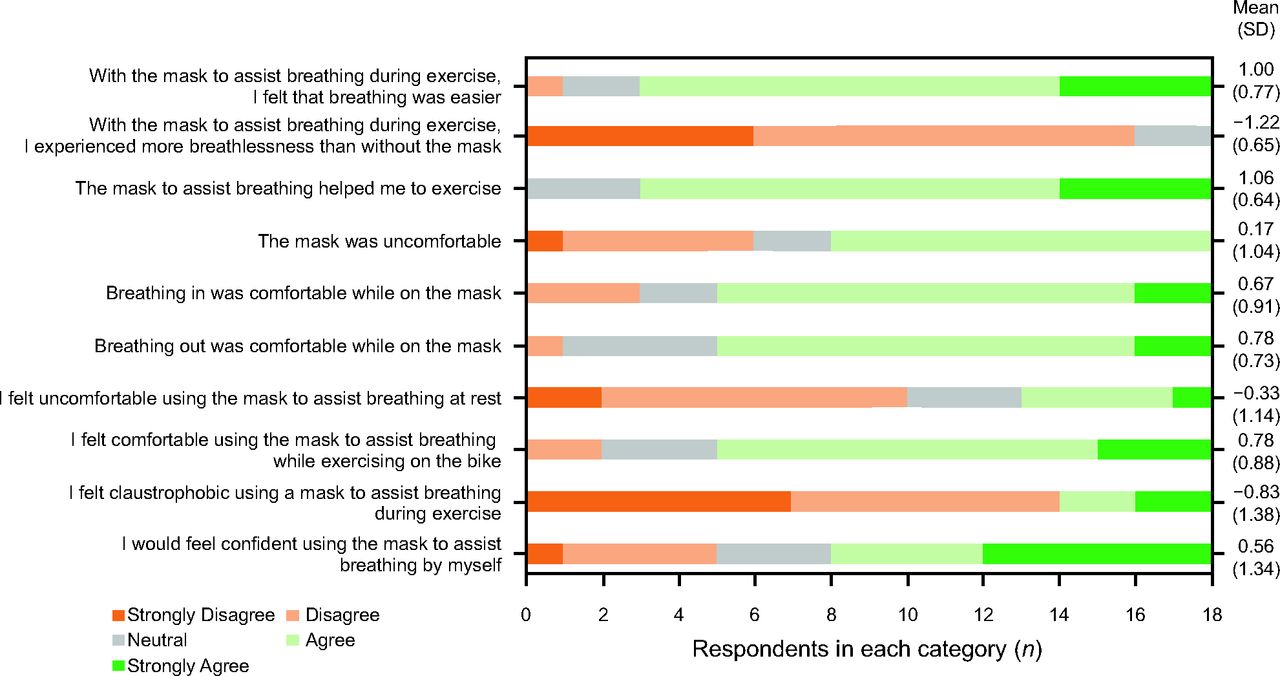
Post-NIV survey responses showed that most participants agreed or strongly agreed that NIV helped them breathe more easily during exercise (15/18, 83%) and that NIV did not increase breathlessness (16/18, 89%). In addition, slightly more than half of the participants agreed that the NIV mask was uncomfortable (10/18, 55%); even so, 55% (10/18) of participants agreed or strongly agreed that they would feel confident using the mask (NIV) by themselves to assist breathing during exercise (Fig. 4).

Post-NIV survey responses. Mean and SD calculated from scored responses. Responses scored as: strongly agree = 2; agree = 1; neutral = 0; disagree = −1; strongly disagree = −2.
Correlations between post-NIV survey questions and baseline characteristics and outcomes from the exercise tests showed a moderate positive correlation between RV/TLC % predicted at baseline and Q1, “With the mask to assist breathing during exercise, I felt that breathing was easier” (ρ = 0.603, P = .02); Q3, “The mask to assist breathing helped me to exercise” (ρ = 0.491, P = .047); and Q8, “I felt comfortable using the mask to breathe during exercise” (ρ = 0.510, P = .033). A moderate negative correlation was found between RV/TLC % predicted at baseline and Q2, “I experienced more breathlessness with NIV” (ρ = − 0.510, P = .031). A moderate negative correlation was also observed between Q2 and the change in exercise duration using NIV with standard EPAP compared to no NIV during exercise (ρ = − 0.588, P = .02). Finally, a moderate positive correlation was found between Q8 and change in IC with titrated EPAP (measured as the difference in the change in IC from baseline to isotime using NIV compared to no NIV, with a large positive difference indicating a greater preservation of IC with NIV) during exercise compared to no NIV during exercise (ρ = 0.488, P = .03) (Table 3, Fig. 5).
Correlations Between Post-Noninvasive Ventilation Survey Responses and Baseline Characteristics and Outcomes From the Exercise Tests
After completion of constant work rate cycle tests on day 2, the most common descriptor of breathlessness selected by participants as most changed by using NIV during exercise was “my breathing requires effort.” Other descriptors of breathlessness, “my breath does not go in/out all the way” and “I can’t get enough air,” also changed with NIV during exercise (Table 2).
Before trialing NIV, no participant selected NIV as their preferred adjunct during exercise; 28% (5/18) selected supplemental O2, and 72% (13/18) selected nothing. After trialing NIV during exercise, 2 participants who previously chose supplemental O2 and 3 participants who chose nothing selected NIV as their preferred adjunct, resulting in 5/18 (28%) selecting NIV, 3/18 (17%) selecting supplemental O2, and 10/18 (55%) selecting nothing.
When asked to select their preferred test of the 3 CETs performed (one without NIV and 2 with NIV), 13/18 participants preferred the exercise test with NIV (8 preferred NIV with standard EPAP, 5 preferred NIV with titrated EPAP), and 5/18 preferred no NIV. Over half (55%) of all participants (10/18) selected the second test using NIV during exercise as their preferred test with NIV.
Interview questions (Table 4) were divided into 4 categories: comfort, ease of use, practicality, benefit. Responses within each category regarding the use of NIV during exercise had words or phrases repeated by multiple participants during the interviews. Examples of common words or phrases for each category are presented below and in Table 5.
Coding and Responses to Semi-Structured Interview Questions
Semi-Structured Interview Questions
Comfort
Participants stated that NIV during exercise was comfortable (7/18 participants); others stated that NIV was comfortable with a caveat (4/18 participants) such as “provided I was in rhythm” (participant 16), and others found NIV during exercise uncomfortable (7/18 participants). The size and weight of the NIV equipment were mentioned as being “uncomfortable” to wear (participant 18) as well as the mask specifically being “too hot” (participant 14) and “not fitting correctly to an open mouth” (participant 7). Common sources of discomfort cited were “leaks” (participant 4) and lack of “sync” (patient-ventilator asynchrony) (participant 13).
Ease of Use
Some participants felt that the ventilator was “unnecessary and complicated” (participant 5) and that they would only use NIV during “supervised training” (participant 14) and “under the direction of professionals to operate the device” (participant 4). The correct fitting of the full-face mask and tubing was also a point of concern for some participants who at times felt they were unsafe (mentioned by 5/18 participants) and potentially unable to remove the mask swiftly without assistance (mentioned by 4/18 participants).
Practicality
The ventilator was seen as large (9/18 participants), bulky (7/18 participants), and not portable (4/18 participants) for use during different activities and exercise. The full-face mask and dual-limb circuit used in this trial were also seen as unusable without assistance outside of clinical settings such as a rehabilitation program (6/18 participants).
Benefit
The benefit from the ventilator in terms of a reduction in breathlessness was reported by 12/18 (67%) of participants, with 2 participants also reporting that they were able to do more exercise with the support from NIV (2/18 participants). All participants agreed NIV could aid exercise (18/18 participants), yet many commented that they themselves were not sick enough to need it (12/18 participants).
Discussion
To our knowledge, this is the first study to report the perceptions of using NIV during exercise in people with COPD who were naïve to NIV and to evaluate the relationship between perceptions of using NIV during exercise and both baseline characteristics and exercise outcomes. The main findings of the study were that participants generally perceived NIV during exercise as beneficial, with greater improvements in exercise endurance time with NIV in those participants who reported higher levels of benefit with NIV. In addition, participants were positive toward using NIV during exercise training in pulmonary rehabilitation. However, many participants found the NIV device bulky and the mask uncomfortable. The present study also demonstrated a moderate positive relationship between the feelings of comfort with NIV during exercise and the degree of both resting hyperinflation and dynamic hyperinflation during exercise.
The perceptions of people using NIV during exercise have not been examined previously. Other studies that have reported the perceptions of people with COPD using NIV have evaluated the use of NIV in the acute care setting during hospitalization for acute respiratory failure or in the home setting with stable patients using long-term nocturnal NIV.16-19 These studies identified the concept of “adapting to NIV,” which often entailed an acclimatization period and a balance between the perceived benefits associated with using NIV and the negative experiences. The health care providers emphasized that individualized social support and personal tolerance to a mask and the NIV apparatus were key factors in the acclimatization to NIV.17 The benefits of an acclimatization period to NIV were also evident in the present study, with over half of participants selecting the second test with NIV as their preferred test overall even though test order was randomized, and no order effects were seen in exercise outcomes between the 2 NIV tests.11 The choice of the second test was potentially due to the learning required to breathe in synchrony with the NIV device, affecting comfort and the perception of benefit. Participants who felt that the second test with NIV was their preferred test stated that they “Started to get used to NIV and … the pressures” (participant 6) or “… stayed in sync more” (participant 3) as reasons for their preference of the second test with NIV rather than a difference in pressure, comfort, or exercise performance. Participants who preferred the first NIV test stated that they were “tired in the second NIV test” (participant 2), which suggested that fatigue may have been an issue.
The present study found significant relationships between participants’ perceptions of NIV and objective measures of exercise with NIV. Specifically, participants who reported that NIV during exercise helped them, exercised for longer with NIV compared with participants who did not report that NIV was beneficial. Participants who had a greater IC at isotime with NIV during exercise likewise responded that they felt comfortable breathing during exercise with NIV. The link between patient perceptions and changes in physiological variables has been reported previously. For example, research investigating airway clearance techniques in patients with cystic fibrosis found that participants’ perception of effective mucus clearance correlated strongly with objective, physiological measures of improved gas exchange.20 However, a recent study examining the use of a handheld portable NIV device, used intermittently to relieve dyspnea during exercise, found that a significant number of participants showed a subjective preference toward the device even though increases in exercise duration or reduction in dyspnea were absent.21 The authors speculated that there may be a psychological desire to have a device that relieves breathlessness.
The semi-structured interviews highlighted several barriers and facilitators to the use of NIV during exercise. Participants stated that the use of NIV during exercise without a health professional to help with the set-up of the device and the circuit was impractical. Participants also commented that when breathing was synchronized with the ventilator, and each breath was supported correctly, it was comfortable to use. However, when breathing synchrony was interrupted by leaks around the mask due to movement, coughing, swallowing, or an unplanned breathing maneuver, it was an effort to return to synchrony, and sometimes this produced enough discomfort to cause cessation of exercise. A previous study in people with severe COPD who were naïve to NIV found that NIV during exercise using a nasal mask failed to improve exercise capacity and exercise endurance time compared to exercise without NIV due to a significant number of patient-ventilator asynchronies secondary to leak.22
A study that documented the experiences of subjects admitted to hospital with acute respiratory failure receiving NIV for the treatment of an exacerbation of COPD found that the support of caregivers in whom they had trust, assistance with equipment setup and configuration, reassurance about the need for NIV, as well as clear directions on use gave them the motivation to continue with NIV.16 In the present study, some participants felt that altering NIV settings or correcting mask leaks to improve synchrony could not be done easily and required assistance. In addition, some participants were concerned for their safety while using a full-face mask as they were unable to doff the mask independently and would not be willing to attempt using NIV alone for fear of suffocation. Participants also reported that the size of the NIV device, associated dual-limb tubing used in the trial and full-face mask, was a limitation to using NIV during exercise. The NIV device and tubing were seen as hard to transport and connect, whereas the mask was cumbersome to put on and take off. Whereas 55% of participants in the post-NIV survey said they would be comfortable to use NIV during exercise, in the interview many participants reported that they would not feel confident using NIV during exercise outside the pulmonary rehabilitation setting.
The current study provides some new information regarding the selection of suitable candidates for NIV during exercise. A relationship between RV/TLC % predicted and the effectiveness of NIV during exercise in people with severe COPD has been previously reported and suggests that individuals with a greater degree of resting hyperinflation are likely to gain greater improvements in exercise capacity from using NIV during exercise.11 The present study demonstrated a link between participants’ perception of benefit with NIV during exercise and the level of resting hyperinflation and improvement in exercise endurance with NIV during exercise. Further, participants with a higher degree of dynamic hyperinflation during an incremental peak exercise test were more likely to perceive a benefit from using NIV during exercise and were more likely to find NIV comfortable to use. This suggests that patients themselves could be a useful source of information when determining whether NIV during exercise is beneficial and, consequently, may be another tool that clinicians can use to assist in the selection of candidates for using NIV during exercise training programs.
The study has some limitations. First, participant perceptions of using NIV during exercise were only sampled on 2 occasions, prior to any experience with NIV and directly following the completion of the exercise tests with NIV. Consequently, the results may not be able to be generalized to individuals who have used NIV during exercise for longer time periods such as during exercise training programs, as perceptions of using NIV during exercise may change over time. Second, as participants were recruited for a trial involving NIV during exercise, it is possible that they were a selected population with a bias toward using NIV or at least with an open mind. Third, in the context of this research trial, participants wore additional equipment, such as a flow sensor attached to the mask to measure metabolic and respiratory variables. This additional equipment may have impacted participants’ perceptions of the bulk and complexity of the equipment required to deliver NIV during exercise. Further, episodes of patient-ventilator asynchrony were not quantified in the present study and may have influenced participants’ perceptions of using NIV during exercise. Additionally, it is unlikely that the findings of the present study are generalizable to individuals with prior experience of using NIV, such as those on domiciliary nocturnal NIV with existing perceptions of NIV, which may influence their experience. Finally, the sample size of the present study was small; and additional factors that could potentially influence participants’ perceptions of using NIV during exercise such as anxiety, depression, and health-related quality of life were not examined.
Further studies are required to investigate the impact of psychological, social, and disease-related factors on the perception of using NIV during exercise in people with COPD and to determine the most effective methods of acclimatizing individuals to using NIV during exercise to improve exercise training program outcomes and completion rates. Future studies should also investigate whether individuals established on nocturnal NIV have a different perception of using NIV during exercise compared with those individuals who are naïve to NIV and to determine how perceptions of using NIV during exercise change over the course of a training program.
Conclusions
Individuals with severe COPD generally had positive perceptions of the use of NIV during exercise for the first time. Participants regarded NIV as being an effective tool to reduce breathlessness during exercise and increase exercise endurance. Participants who perceived a greater improvement with NIV during exercise were more likely to have an actual increase in exercise duration with NIV during exercise compared to exercise without NIV. Participants did not believe that NIV during exercise could be used without assistance and supervision.
Acknowledgments
We would like to thank Dr Rob Heard for assistance in analysis of qualitative data.
Footnotes
- Correspondence: Clancy J Dennis BEng, c/o Jennifer Alison, University of Sydney, Faculty of Medicine and Health, Camperdown, Sydney 2006, Australia. E-mail: cden2754{at}uni.sydney.edu.au
The authors have disclosed no conflicts of interest.
This work received no funding.
A version of this paper was presented by Clancy Dennis at the American Thoracic Society Conference held virtually May 1, 2020.
- Copyright © 2022 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}