

Abstract
BACKGROUND: In patients being considered for lung-resection surgery, quantitative perfusion scintigraphy is used to predict postoperative lung function and guide the determination of lung-resection candidacy. Vibration-response imaging has been proposed as a noninvasive, radiation-free, and simpler method to predict postoperative lung function. We compared vibration-response imaging to quantitative perfusion scintigraphy for predicting postoperative FEV1 and diffusing capacity of the lung for carbon monoxide (DLCO).
METHODS: We enrolled 35 candidates for lung resection. Twenty-five patients had preoperative FEV1 and DLCO measurements.
RESULTS: The vibration-response-imaging measurements showed strong correlation with the quantitative-perfusion-scintigraphy measurements of predicted postoperative FEV1% (r = 0.87, P < .001), predicted postoperative FEV1 (r = 0.90, P < .001), and predicted postoperative DLCO% (r = 0.90, P < .001). There was a correlation between predicted postoperative FEV1 (% and L) measured via quantitative perfusion scintigraphy and the actual postoperative FEV1 (% and L) (r = 0.47, P = .048, r = 0.73, P < .001). There was no difference between the vibration-response-imaging measurements and the actual postoperative measurements of predicted postoperative FEV1 (% and L). There was a correlation between predicted postoperative FEV1 (% and L) measured via vibration-response imaging and actual postoperative FEV1 (% and L) (r = 0.52, P = .044, r = 0.79, P < .001). The mean differences between the predicted and actual postoperative FEV1 values were 49 mL with vibration-response imaging, versus 230 mL with quantitative perfusion scintigraphy. Neither the vibration-response imaging nor the quantitative perfusion scintigraphy predicted postoperative DLCO% values agreed with the actual postoperative DLCO% values.
CONCLUSIONS: Vibration-response imaging may be a good alternative to quantitative perfusion scintigraphy in evaluating lung-resection candidacy.
- vibration-response imaging
- quantitative perfusion scintigraphy
- lung resection
- preoperative evaluation
- lung function
- lung carcinoma
Introduction
Postoperative complications and mortality following lung resection are high.1–6 Various pulmonary function tests have been used to assess the operability of patients and to predict morbidity and mortality after surgery.1,5,6 In lung-resection candidates who have percent-of-predicted FEV1 and/or percent-of-predicted diffusing capacity of the lung for carbon monoxide (DLCO) < 80%, actual postoperative lung function should be measured via additional tests.1,5 Quantitative radionuclide ventilation-perfusion studies are commonly used to predict postoperative lung function and outcome.1,5,7–9 In recent years, simpler and radiation-free methods to predict postoperative lung function have been researched.10–12 Vibration-response imaging measures acoustic vibratory energy at the chest wall, generated by breath sounds during spontaneous breathing.13,14 The signals are processed to generate a dynamic lung image that can be quantified and used to calculate lung function, similar to perfusion or ventilation lung scintigraphy.15,16 Previous limited studies found correlation between measurements via vibration-response imaging and via quantitative radionuclide ventilation-perfusion scintigraphy.15,16
The primary objective of the present study was to prospectively investigate the agreement between predicted postoperative FEV1 and DLCO via vibration-response imaging and actual postoperative FEV1 and DLCO values after lung resection. The secondary aim was to evaluate the correlation between predicted postoperative vibration-response-imaging measurements and predicted postoperative quantitative-perfusion-scintigraphy measurements.
Methods
The study was approved by the ethics committee of the Istanbul Medical Faculty, Istanbul University, and written informed consent was obtained from all patients. This was a prospective study. We screened all candidates for lung resection who were admitted to the Pulmonary Department, Istanbul Medical Faculty, Istanbul University, between March and September 2009. The patients underwent lung-function evaluation prior to, and 4–8 weeks after lung resection. We measured preoperative and predictive postoperative FEV1, FEV1%, and DLCO%, via vibration-response imaging and quantitative perfusion scintigraphy. We also recorded the patients' demographics and medical histories. Spirometry and DLCO (corrected for hemoglobin) were measured (ZAN 740N, nSpire Health, Oberthulba, Germany) according to American Thoracic Society guidelines.17 The exclusion criteria were lung resection less than lobectomy; factors that interfered with recording or sensor adhesion (chest-wall or spine deformities such as severe scoliosis or kyphosis, hirsutism, contagious skin lesion, cardiac pacemaker, or implantable defibrillator, body mass index < 19 kg/m2); active lower-respiratory-tract infection; and non-cooperation in regular inspiration and expiration.
Radionuclide Quantitative Perfusion Scintigraphy
We performed quantitative perfusion scintigraphy with technetium-99m macro-aggregated albumin 1 or 2 days before surgery, with the patient seated upright. We calculated predicted postoperative FEV1, FEV1%, and DLCO% with the Kristersson formula.18
Vibration-Response Imaging
We performed vibration-response imaging (VRIxp, Deep Breeze, Or-Akiva, Israel) 1 or 2 days before surgery, with the patient seated in a quiet environment. The VRIxp system quantifies breath sounds and depicts the findings as a dynamic image, as described previously.14 According to the patient's height (7-row array for patients ≥ 165 cm, 6-row array for patients < 165 cm), either 21 or 18 piezoelectric contact sensors are used for recording. The sensors are attached symmetrically to the patient's back, beginning 1.5 cm below the scapula, with a 3–6 cm space between each sensor. Airway secretions can interfere with the vibration-response imaging results, so before the acoustic measurements we had the patient cough, huff, and/or conduct forced expiratory technique to clear secretions. With the room silent, we instructed the patient to inhale deeply and exhale without force via the mouth, for 12 seconds, during which we recorded at least 3 respiratory cycles with uniform graphs. We obtained at least 3 satisfactory recordings from each patient, and analyzed the recording with the best technical quality, determined by a computer algorithm. The analysis of the vibration-response imaging was done by a physician. The quantitative lung data were automatically calculated as the average total energy within the upper and lower lung regions for the left and right lungs. We used the regional quantitative lung data and the formulas for prediction of postoperative lung function to calculate FEV1, FEV1%, and DLCO%.
Statistical Analysis
We present the FEV1 and DLCO values as mean ± SD. We used the Wilcoxon signed-rank test for paired data to analyze differences between the values. Differences were considered significant when P < .05. We used the Bland-Altman method19 to evaluate the agreement between the actual and predicted postoperative values. We calculated Pearson correlation coefficients to evaluate the relationship between predicted postoperative measurements via vibration-response imaging and quantitative perfusion scintigraphy.
Results
We included 35 lung-resection candidates (mean age 55.3 ± 11.6 y, age range 28–75 y). Twenty-seven patients were male. The diagnoses were: multiple-drug-resistant tuberculosis (1), non-small-cell carcinoma (13), neuroendocrine carcinoma (1), squamous cell carcinoma (8), adenocarcinoma (10), pulmonary metastasis (2). Eighteen patients had comorbidities: COPD (6), ischemic heart disease (1), diabetes mellitus (2), hypertension (9). Bronchoscopy showed endobronchial mass in 15 patients. None of the endobronchial masses were located in the main bronchus, and all caused partial bronchial obstruction. We excluded 10 patients: 4 because of inoperability based on lung-function tests, 1 refused surgery, and 5 had vibration-response-imaging recording problems, such as artifacts, less than 3 breathing cycles in 12 seconds, and ambient noise.
Preoperative correlation analysis was based on 25 patients for FEV1 (% and L) and 22 patients for DLCO%. Of these 25 patients, 1 refused surgery and 24 had lung resection (5 pneumonectomy, 19 lobectomy). Three patients died postoperatively, 1 from pneumonia, and 2 from arrhythmia. One patient refused postoperative evaluation. Therefore, 20 patients (4 pneumonectomy, 16 lobectomy) underwent postoperative lung function evaluation.
Eight patients had postoperative complications: 2 pneumonia, 2 arrhythmia, 2 fistula at the operation side, and 2 pneumothorax. Three patients died in the hospital. In total, 4 patients had died 3 months after lung resection.
Correlation of Predicted Postoperative Values
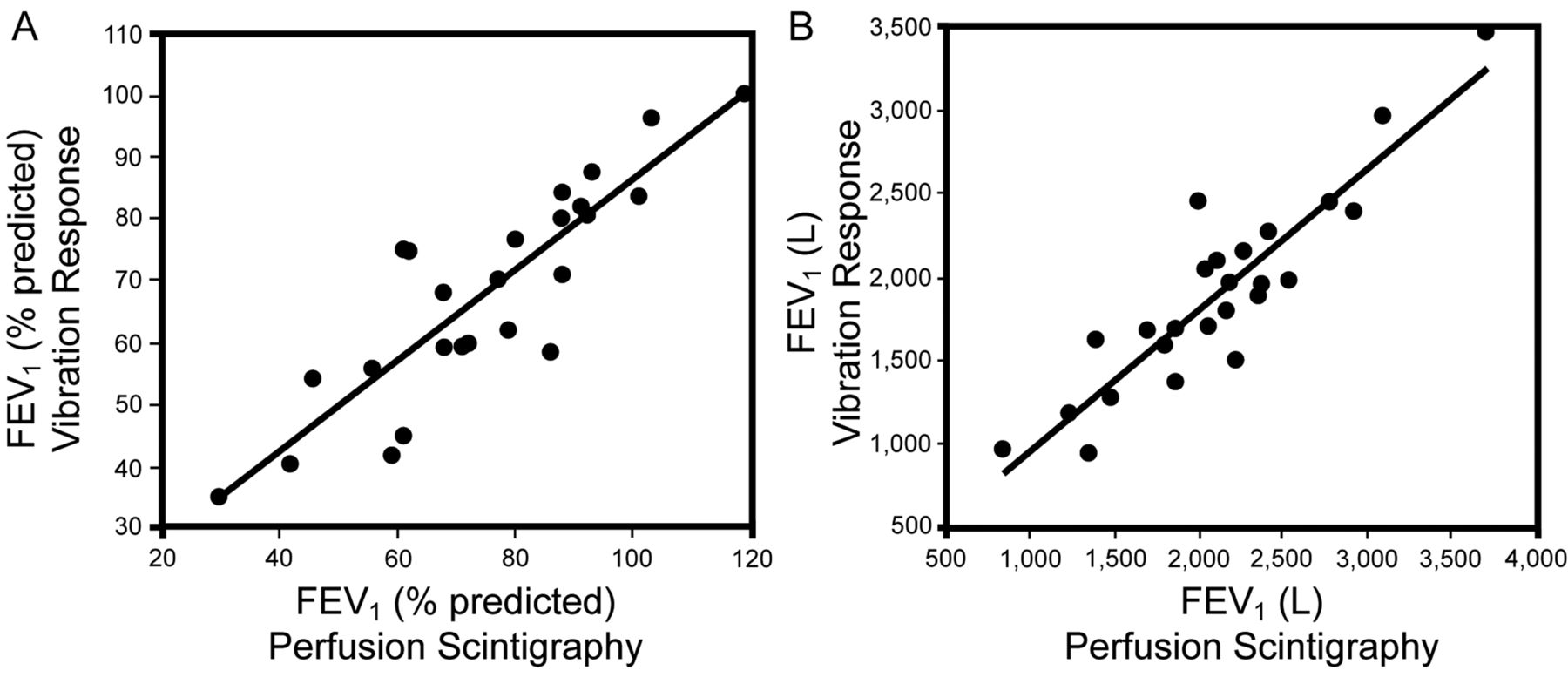
Table 1 shows the average postoperative pulmonary function test results and the correlations between vibration-response imaging and quantitative perfusion scintigraphy measurements. FEV1, FEV1%, and DLCO% via vibration-response imaging were lower than via quantitative perfusion scintigraphy. There was a significant difference between the average predicted postoperative FEV1, FEV1%, DLCO% values via quantitative perfusion scintigraphy versus vibration-response imaging (P < .001 for all 3 differences). The predicted FEV1%, FEV1, and DLCO% values via vibration-response imaging correlated well with the quantitative perfusion scintigraphy values (r = 0.87, P < .001, r = 0.90, P < .001, r = 0.90, P < .001, respectively) (Fig. 1). The Bland-Altman analysis (Fig. 2) shows the agreement between FEV1 and FEV1% via vibration-response imaging and via quantitative perfusion scintigraphy.
Average Postoperative Pulmonary Function Test Results and Correlations Between Vibration-Response Imaging and Quantitative Perfusion Scintigraphy Measurements

Correlation of predicted postoperative FEV1 and percent-of-predicted postoperative FEV1 measured via quantitative perfusion scintigraphy versus via vibration-response imaging.

Bland-Altman plots of predicted postoperative FEV1 and percent-of-predicted postoperative FEV1 measured via vibration-response imaging versus via postoperative spirometry.
Predicted Versus Actual Postoperative FEV1 and DLCO
We analyzed the predicted versus actual postoperative values from 20 subjects (8 with endobronchial mass). Table 2 shows the mean ± SD actual preoperative, predicted postoperative, and actual postoperative values. There were significant differences between predicted postoperative FEV1 (% and L) via quantitative perfusion scintigraphy versus via postoperative spirometry (P = .049, and P = .047 respectively). There was a correlation between predicted postoperative FEV1 (% and L) via quantitative perfusion scintigraphy and actual postoperative FEV1 (% and L) (r = 0.47, P = .048, and r = 0.73, P < .001, respectively). The differences between predicted postoperative FEV1 (% and L) via vibration-response imaging versus postoperative spirometry were not significant. There was a correlation between predicted postoperative FEV1 (% and L) via vibration-response imaging and actual postoperative FEV1 (r = 0.52, P = .044, and r = 0.79, P < .001, respectively). There was also agreement between the vibration-response-imaging values and the postoperative spirometry values. The mean difference between the predicted and actual postoperative FEV1 was 49 mL with vibration-response imaging, and 230 mL with quantitative perfusion scintigraphy. The differences between predicted and actual postoperative DLCO were significant (P < .001) for both quantitative perfusion scintigraphy and vibration-response imaging. The Bland-Altman analysis showed no agreement between predicted and actual postoperative DLCO values.
Pulmonary Function Test Results (no. = 20)*
Discussion
Quantitative perfusion scintigraphy is the most commonly accepted and best validated technique for predicting lung function after lung resection.5,7–11 Based on this fact, we compared the accuracy of vibration-response imaging and quantitative perfusion scintigraphy to guide patient selection for lung resection. There was good correlation between the predicted postoperative FEV1%, FEV1, and DLCO% values via quantitative perfusion scintigraphy and vibration-response imaging. These results are similar to those in limited previous studies of vibration-response imaging.15,16 Jimenez et al found that average predicted postoperative lung-function values were similar for quantitative perfusion scintigraphy and vibration-response imaging (correlation 0.74, concordance 0.70).16
Further, we found a good correlation between predicted postoperative FEV1 (% and L) via vibration-response imaging and the actual postoperative values, consistent with the findings of Jimenez et al.16 We also found that the predicted postoperative FEV1 values via quantitative perfusion scintigraphy and vibration-response imaging were more reliable to assess actual postoperative values than FEV1%. To our knowledge, our study is the first to find the best correlation between predicted postoperative FEV1 via vibration-response imaging and actual postoperative FEV1 (r = 0.79).
The predicted FEV1 (% and L) values via quantitative perfusion scintigraphy were significantly higher than the actual postoperative values, whereas there was no significant difference between the predicted FEV1 via vibration-response imaging and the actual postoperative FEV1. In the study by Jimenez et al, vibration-response imaging showed high accuracy in predicting post-lung-resection FEV1.16 In that study the predicted values via vibration-response imaging and actual postoperative FEV1 values were similar to each other, as in our results.
An important finding in our study was that the mean difference between predicted postoperative FEV1 via quantitative perfusion scintigraphy and actual postoperative FEV1 was 230 mL. Such a big difference may be very important in the decision of whether or not to proceed with lung resection, especially in patients with limited lung function. The difference between actual postoperative FEV1 and predicted postoperative FEV1 via vibration-response imaging was 49 mL, so vibration-response imaging may be more reliable than quantitative perfusion scintigraphy in the lung-resection decision.
According to the American College of Chest Physician guidelines, in patients undergoing evaluation for lung cancer resection, DLCO is recommended for patients with percent-of-predicted FEV1 < 80%, unexplained dyspnea, or diffuse parenchymal disease on radiograph.1 Additionally, several investigators have documented the usefulness of DLCO for predicting the risk of complications and postoperative mortality.20–23 In our study we found a good correlation between predicted DLCO via quantitative perfusion scintigraphy and DLCO via vibration-response imaging. However, there was no agreement between the actual postoperative values and the predictions via quantitative perfusion scintigraphy or vibration-response imaging.
Interestingly, we found no significant decrease in DLCO after lung resection. This finding was also mentioned in previous studies.24,25 Wang et al reported that DLCO did not significantly decrease after lobectomy but decreased after pneumonectomy at postoperative first year.26 In our study the high number of lobectomy patients might explain the preserved DLCO. Another explanation may be resection of hyperinflated nonfunctional lung parenchyma in COPD patients.27 In our study, 2 patients with postoperative DLCO increase had COPD according to the Global Initiative for Chronic Obstructive Lung Disease criteria.17 Furthermore, we thought that resection of tumor mass would improve unequal ventilation and parenchymal shunt, resulting in better DLCO%.
In our study 8 patients had postoperative complications, 3 patients had died after the first month, and 4 patients had died at the third month. Those mortality rates are similar to other studies.28–31
Limitations
We included few subjects. We should have performed postoperative evaluation not only at 4–8 weeks but also at 3 months. And because we had so few subjects with pneumonectomy, we could not compare the results from the lobectomy and pneumonectomy patients.
Recently, a few studies of vibration-response imaging have included descriptions of vibration-response images in healthy subjects and subjects with various lung pathologies.14,32–34 Vibration-response imaging measures acoustic energy, not lung perfusion or ventilation. However, predicted postoperative lung function via vibration-response imaging is analogous to quantitative lung scintigraphy. Vibration-response imaging is also time-saving and radiation-free.
Conclusions
Prediction of postoperative lung function via vibration-response imaging is better than via quantitative perfusion scintigraphy. Vibration-response imaging may play an important role in predicting postoperative lung function. Like the 2 previous studies15,16 of vibration-response imaging, our cohort was small, so a larger study is needed. Vibration-response imaging is a simple, noninvasive, radiation-free, bedside method that can be used instead of quantitative perfusion scintigraphy for assessing predicted postoperative lung function of thoracic surgery candidates.
Footnotes
- Correspondence: Esen Kiyan MD, Department of Pulmonary Diseases, Istanbul Medical Faculty, Istanbul University, Posta Kodu 34 390, Istanbul, Turkey. E-mail: ekiyan{at}istanbul.edu.tr.
The authors have disclosed no conflicts of interest.
- Copyright © 2011 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}