

Abstract
BACKGROUND: CPAP is considered to be the cornerstone of therapy for obstructive sleep apnea. However, adherence to this treatment is frequently poor, which may lead to ongoing symptoms, including daytime sleepiness and poor cognitive function. We aimed to determine the efficacy of showing patients their raw graphic polysomnography (PSG) data in increasing their CPAP adherence.
METHODS: The subjects were patients with obstructive sleep apnea (n = 37, diagnosed on prior PSG), who were prospectively randomized into an experimental arm or a control arm. The patients in the experimental arm (n = 18) were shown detailed PSG data, including graphic data from PSG prior to prescription of CPAP. The patients in the control arm (n = 19) were shown the non-graphic paper report of the PSG. Adherence data, collected using CPAP devices with internal microprocessors (adherence cards), was read at 4 weeks after treatment initiation.
RESULTS: There was no difference in age (57.3 ± 11.8 y vs 55.5 ± 11.6 y, P = .64), body mass index (BMI) (32.7 ± 6.3 kg/m2 vs 32.3 ± 6.6 kg/m2, P = .85), and apnea-hypopnea index (36.0 ± 27.8 events/h vs 30.5 ± 19.1 events/h, P = .48) between the experimental and control arms. There was no difference in percent of days CPAP was used (58% vs 64%, P = .59) and average number of hours each night CPAP was used (3.9 ± 2.1 h vs 4.1 ± 2.5 h, P = .76) between the experimental and control arms, respectively. In multi logistic regression models, which included age, BMI > 30 kg/m2, apnea-hypopnea index, and experimental intervention, only BMI was found to increase likelihood of improved adherence (odds ratio = 13.3, P = .007).
CONCLUSIONS: Showing patients raw graphic PSG data does not seem to improve adherence to CPAP. BMI is a very strong predictor of CPAP adherence.
Introduction
Obstructive sleep apnea (OSA) is a highly prevalent disorder. The Wisconsin Sleep Cohort Study showed the estimated prevalence of OSA to be 4–9% for women and 9–24% for men.1 It has been associated with or is causal of serious chronic illnesses such as hypertension,2 obesity, diabetes, myocardial infarction, heart failure, and stroke.3 Despite the high efficacy of CPAP in reversing upper-airway obstruction in sleep apnea, treatment effectiveness is limited by variable adherence to prescribed therapy. When adherence is defined as > 4 hours of nightly use,4 46–83% of patients with OSA have been reported to be non-adherent to treatment.5
Patients have difficulty adhering to treatment owing to one or more of the side effects, such as pressure intolerance,6 claustrophobic reaction to the mask, mask dislodgement, and machine noise.7
Several interventions can potentially improve adherence; intensive support to the patient with home visits,8 one time use of hypnotics during titration polysomnogram (PSG),9 upper airway surgery in select patients,10 C-Flex,11 sharing bed with partner,12 and subjective improvement in sleep quality on titration study.13
The extent to which individuals believe they can control events that affect them impacts their adherence to medical treatment. A recent study suggested that individuals who discontinued CPAP could not be convinced of the necessity of CPAP by physicians or nurses, due to their reduced external control belief (belief that environment controls their life).14 Cognitive therapy can affect control belief.15 Previously studied cognitive interventions shown to positively impact CPAP adherence involved showing patients educational material on a screen (eg, a discussion of misconceptions about sleep apnea,16 video of OSA events17), followed by allowing patients to ask questions during individual or group sessions.18 Thus we intended to observe the effect of visualizing PSG raw graphic data on a computer screen on adherence to pressure therapy, as a similarly devised but more practical approach in the clinical setting; we conducted a prospective, randomized, placebo-controlled trial. At our institution showing the paper report to the sleep apnea patient after their PSG is standard practice. We hypothesized that viewing actual PSG graphic data by the patient would improve adherence to positive airway pressure therapy, when compared with standard care.
QUICK LOOK
Current knowledge
CPAP is the cornerstone of therapy for obstructive sleep apnea, but patient adherence to CPAP is frequently poor, which may lead to continued symptoms, including daytime sleepiness and poor cognitive function.
What this paper contributes to our knowledge
Showing the patients the raw graphic polysomnography data did not improve patient adherence to CPAP. Greater body mass index predicted better CPAP adherence.
Methods
This study was a prospective randomized clinical trial. Each subject had a diagnostic sleep study documenting sleep apnea, followed by a titration study to determine optimal pressure setting. All subjects who underwent PSG and were found to have OSA at the James A Lovell Federal Health Care Center, North Chicago, were screened and enrolled between June 2010 and August 2010. Per sleep center protocol, all subjects received their out-patient medications on the night of their PSG. A central electroencephalogram derivation was included in all PSG recordings. Electromyogram was used to record chin and leg movements. Chest and abdominal movements were recorded by impedance bands. Air flow was assessed using both nasal pressure transducer and thermistor methods. We excluded patients with legal blindness, intellectual disability, or who opted for sleep apnea treatment by surgery or oral device. The study protocol was approved by the James A Lovell Federal Health Care Center's institutional review board. Informed consent was obtained from each subject.
OSA was defined as present if the apnea-hypopnea index (AHI) was > 5 events/h, and severe OSA was defined as AHI > 30 events/h. Apnea, hypopnea, and OSA were defined per the American Academy of Sleep criteria.19 The recommended definition for hypopnea was used.
Baseline characteristics, including age, sex, height, weight, body mass index (BMI) and Epworth Sleepiness Scale score, were recorded at the first visit. Clinicians taking care of patients prescribed pressure therapy. As a standard of care at our Department of Veterans Affairs hospital, all equipment was provided to the patients free of cost. Respiratory therapists educated all patients about the use and maintenance of the CPAP machine (standard practice in our clinic), but not about OSA. These education sessions occurred after the patients were diagnosed with OSA. Randomization was achieved by the patient picking up an envelope from a stack, which had a concealed assignment code: zero for non-graphic, paper report, and 1 for graphic report. The envelope was not replaced in the stack. Physicians (RN and LS) showed the studies to the subjects in an additional dedicated session. These physicians were not blinded, for the obvious reason that the graphic study was on a computer screen, while the paper report was on sheets of paper.
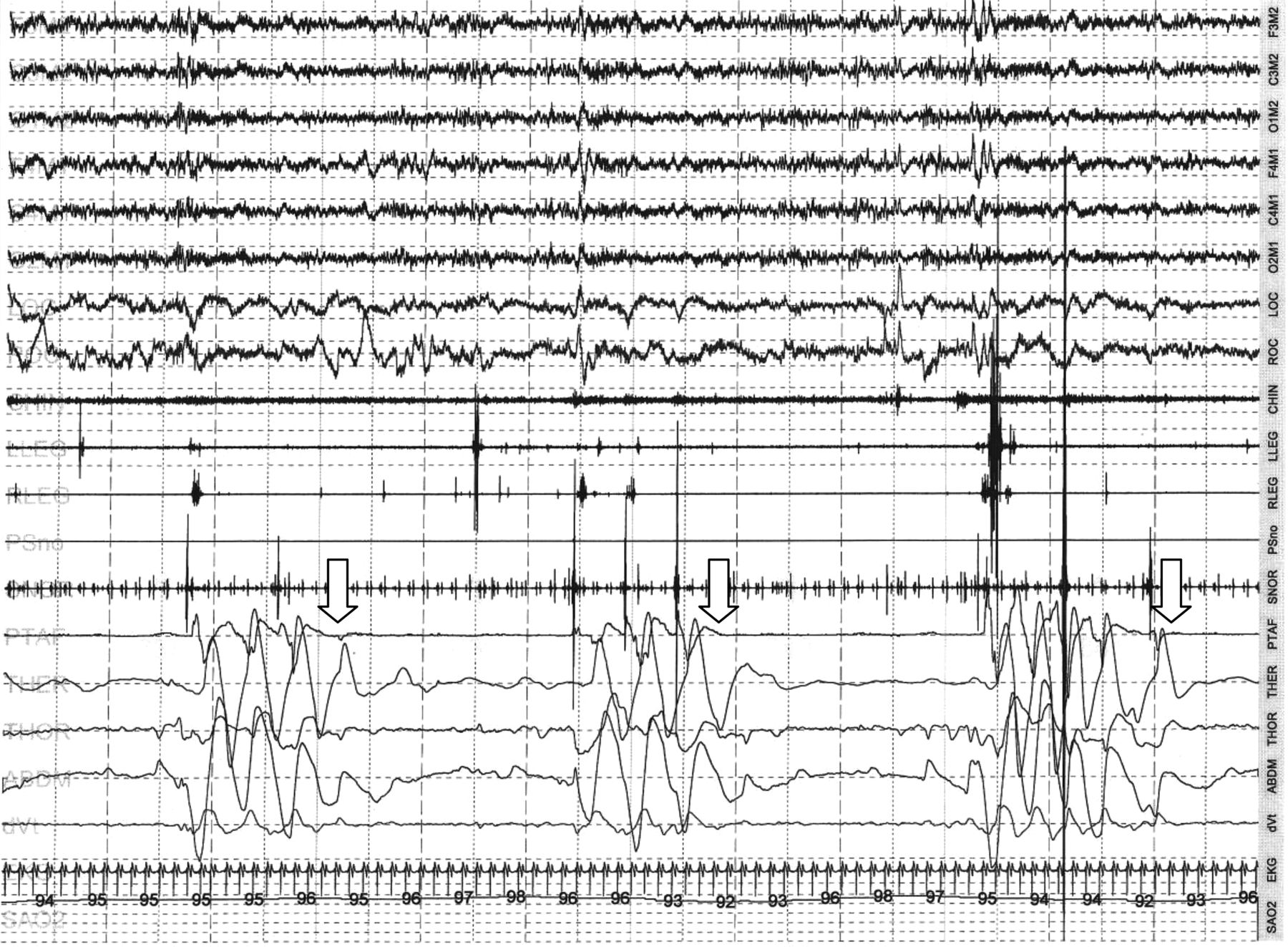
The data of his or her diagnostic sleep study were shown and explained to each subject, either on computer (SomnoStar Pro 7-3A, CareFusion, San Diego, California) or non-graphic, paper report generated by same system. The graphic study was displayed on the computer screen in 2 minute epoch windows showing the electroencephalogram, and respiratory data of the subjects' snoring, apnea, and oxygen saturations, and was explained to the subject in standardized fashion (Fig. 1). The non-graphic, paper report review involved showing a 3 page report that showed sleep efficiency, architecture, AHI, desaturations, arousals, effect of position, cardiac rhythms, and periodic limb movement disorder, in numerical form (Fig. 2). Subjects were then asked to repeat what they had learned during the session. Subjects was encouraged to ask questions, and answers were also provided in a standardized manner. Each review session was timed and lasted 15 min.

Sample of 2 minutes from a polysomnography of a patient with severe obstructive sleep apnea, with measurement of ocular channels (LOC, ROC), electroencephalograph channels (C4M1, F4M1, O1M2, C1M2, F3M2), chin (CHIN) and leg electromyogram channels (LLEG,RLEG), electrocardiogram (ECG), nasal flow (PTAF), snoring (SNOR), oxygen saturation by pulse oximetry (SAO2), and chest (THOR) and abdomen (ABDM) bands. Arrows mark the obstructive events.

Sample of 3 page paper report showing sleep efficiency, architecture, apnea-hypopnea index, desaturations, arousals, effect of position, cardiac rhythms and periodic limb movement disorder in numerical form.
Usual respiratory therapist follow-up as part of clinical care included a follow-up call after 1 week, to identify any issues with therapy and to resolve them and to re-emphasize adherence. These therapists were unaware of the subjects' study enrollment.
At the 1 month follow-up visit, the adherence data card was removed from the CPAP device and data were downloaded onto a computer using proprietary software (Encore, Respironics, Murrysville, Pennsylvania) provided by the manufacturer of the CPAP device, and adherence data were collected. The following were recorded and calculated from these data: number of days machine used, percent of days machine used, and average hours of use on the days when machine was used. The adherence card from the machine records the machine in use only when it is on and running at pressure. Adherence cards have been validated in an earlier study as an objective measure of CPAP use.20 We defined adherence to treatment as the subject's use of CPAP ≥ 4 hours a night for > 70% of nights, based on expert guidelines.21 Subjects were aware of the fact that this card records adherence to therapy.
Statistical Analysis
We estimated that a total of 20 subjects (10 in each arm) would be required to demonstrate a change of 1 hour in mean usage time, with a power of 0.8 and α error equal to .05. A previous study looking at other cognitive interventions have used similar sample size and demonstrated similar mean difference.22 We recruited 20 subjects, and analysis of those did not show a statistically significant result. A recent systemic review23 looking at the effect of cognitive interventions on CPAP adherence showed a net mean difference of 0.59 hours. It was hypothesized that if the effect size was smaller than anticipated, it would be missed, and so the sample size was increased. Our final sample size was 40 subjects, 20 in each arm. The data were normally distributed, and the Student t test was utilized to compare the 2 groups, as appropriate. We used multiple logistic regression analysis to calculate the influence of intervention on adherence while adjusting for parameters previously shown to change adherence. Additionally, we calculated the effect of all parameters individually on adherence. We used statistics software (Epi-info, Centers for Disease Control and Prevention, Atlanta, Georgia) to analyze data. A P value of < .05 was considered significant.
Results
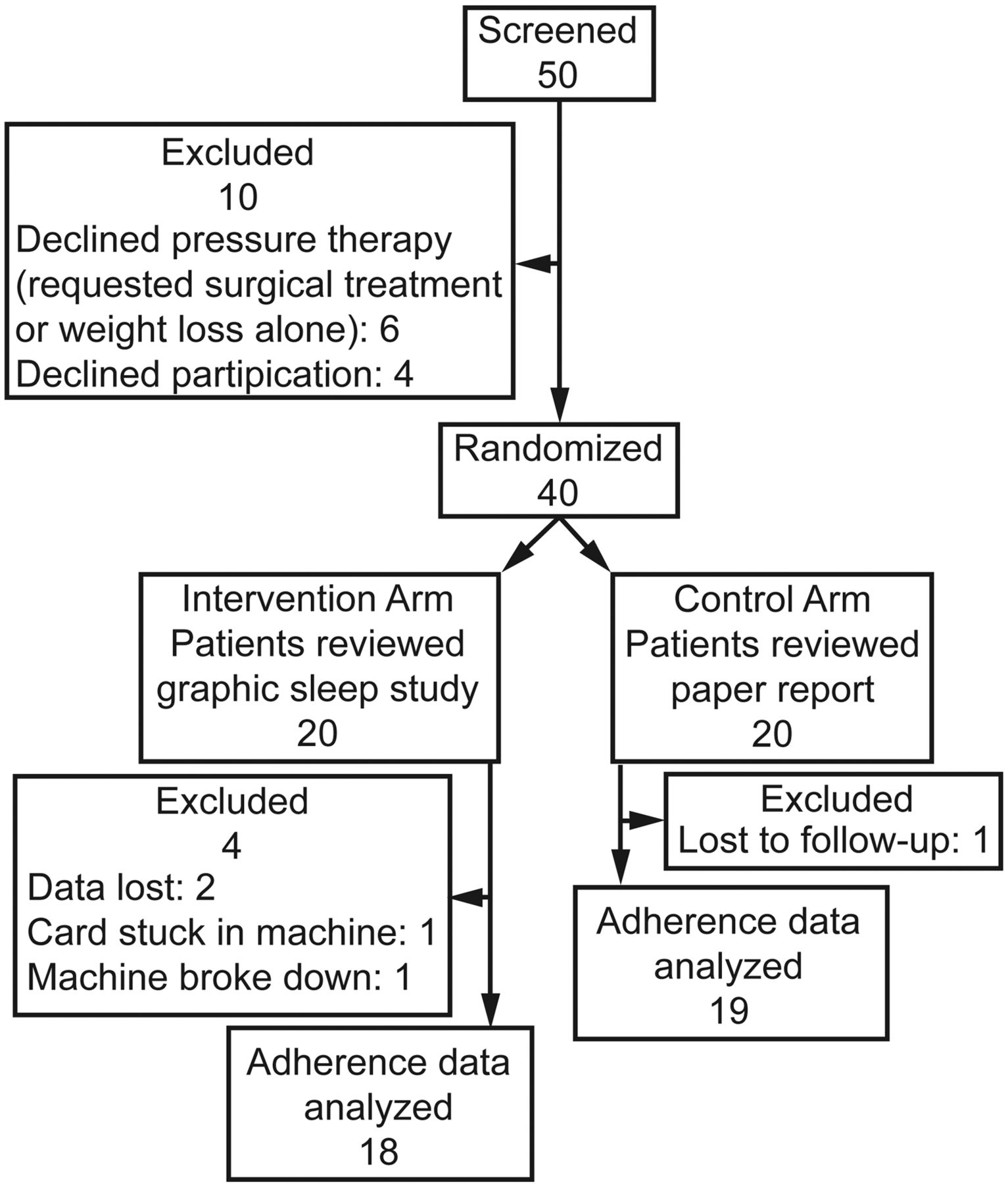
A total of 50 patients were screened. Forty of them agreed to participate (Fig. 3). Forty subjects were randomized to see the raw graphic sleep study (n = 20) or paper report (n = 20). Due to technical difficulties, data of 3 subjects could not be obtained; 37 subjects' adherence data were available. The mean age of our subject population was 56.4 ± 11.6 years, and 87% were male. Mean BMI was 32.6 ± 6.4 kg/m2, and mean AHI was 33.2 ± 23.5 events/h. The mean Epworth Sleepiness Scale score was 9.9 ± 5.2.

Screening, recruitment, randomization, and analysis.
Baseline characteristics were not different between the experimental and control arms (Table 1). Comparison of adherence data did not show a difference between the experimental and control arms (Table 2). In a multi-logistic regression model (n = 37), which included age, BMI, AHI, Epworth sleepiness scale score, and the experimental intervention, only BMI was found to increase the likelihood of improved adherence (P = .004). For BMI > 30 kg/m2, the odds ratio for adherence was 13.3 (P = .007) (Table 3).
Cohort Characteristics Stratified by Subjects' Review of Their Sleep Study
Adherence to CPAP
Odds Ratios for Adherence to CPAP in All 37 Subjects
Discussion
In our study the intervention (seeing raw graphic PSG data) did not improve adherence, when compared to standard practice (showing a non-graphic, paper report). There are several possible reasons for this result. First, despite our efforts to eliminate the complexity and difficulty in understanding the graphic data, as mentioned in methods, it may be more complicated than the paper report and did not improve subjects' perception or understanding about their sleep problem and importance of treatment. Although no objective measurement of subjects' understanding was collected, subjects were asked to repeat what they had learned during the sessions. Second, our study was powered to detect a difference of 1 hour in CPAP usage per night, and, although unlikely, a smaller, yet clinically important, difference could have been missed. Third, we did not include the interface data, which is also a modifier of adherence to pressure therapy.24 Whether or not an individual is motivated internally or externally (locus of control) to engage in healthy behaviors has been examined as a predictor of CPAP adherence at 1 year.13 It is plausible that those who discontinued treatment were less externally motivated, suggesting that they would be less receptive to cognitive interventions. However, any impact on subjects' perception of CPAP or locus of control was not measured. Also our cohort had a mean Epworth Sleepiness Scale score of 9. This may have adversely impacted adherence in both groups.24 Lastly, both methods (graphic vs non-graphic, paper report) may be equally effective.
The adherence rates were 38% and 47% in the treatment group and control group, respectively. These results are comparable with the previous studies reported in the literature (17–54% adherence).25
A multi-regression analysis including all subjects demonstrated that only BMI predicted CPAP adherence in the initial 4 weeks of treatment. No other variables (age, sex, AHI, degree of sleepiness) predicted adherence.
Some studies have found relationships between age, sex, severity of disease, and symptoms of sleepiness to subsequent adherence to CPAP therapy.8,10 Other studies have not found such relationships.26–29 Our study shows only BMI as a significant predictor of adherence. Some studies showed higher BMI suggests adherence.9,25 It is plausible that the effect of severity of disease and severity of symptoms on adherence to CPAP is confounded by BMI. However, many studies did not show a relationship between BMI and CPAP adherence.8,10,27
Obesity impairs ventilatory mechanics,30,31 increases the work of breathing32 and carbon dioxide production, results in respiratory muscle dysfunction, and reduces ventilatory response to hypercapnia, resulting in hypoventilation.33 The prevalence of obesity hypoventilation syndrome is high (up to 30%) in patients with OSA.34 Treatment of hypoventilation with positive airway pressure improves chronic daytime hypercapnia, hypoxia, excessive daytime sleepiness and wakefulness, and dyspnea,35–40 and this improvement is directly related to the daily dose of CPAP therapy.4,41 Although we did not check plasma carbon dioxide levels, we postulate that this could explain improved patient adherence in a substantially obese patient subset with coexistent hypoventilation. However, further investigation is needed to explain the association of CPAP adherence to BMI.
Our intervention compares well to other cognitive interventions described in the literature. These include education sessions on consequences of OSA and efficacy of CPAP,42 sessions of cognitive behavioral therapy, including videos of actual OSA patients,43 and increased education on a one on one basis.16,44,45 Similar to our intervention, others involved showing patients educational material on a screen (discussion of misconceptions about sleep apnea,16 video of OSA events,17 et cetera), followed by allowing patients to ask questions during individual or group sessions.18
Although this research was designed as a prospective, randomized, controlled clinical study, there are some limitations. We did not record interface (mask) and comorbid condition such as insomnia or post-traumatic stress disorder in our patient population, which may also be important determinants of adherence.46 Our study cases were selected from a specific population (ie, mostly middle age male veterans). The incidence of post-traumatic stress disorder is high in this population.47 Not controlling for the effect of auto PAP versus CPAP may affect findings. However, it is unclear if the type of PAP therapy affects adherence.48 It is impossible to completely prevent confounding when variables are so intricately linked as BMI and AHI.4 However, a multi-logistic regression model should adjust for any confounders. It is possible that the duration of the intervention was too short. Our study was directed at identifying a clinically relevant, effective, and practical approach to improving adherence. A duration of 15 min was considered practical in a clinical setting. It is possible that longer sessions could result in improvement in adherence. Indeed, a significantly more labor intensive cognitive intervention has been shown to improve CPAP adherence.49 However such time consuming interventions are not practical in the everyday clinical setting.
Nonetheless, to our knowledge this is the first randomized, controlled trial directly addressing the issue. The negative result suggests that other factors affecting CPAP adherence may be more important. Larger prospective, controlled, randomized studies are needed to address the role of cognitive interventions in determining adherence to therapy.
Conclusions
In conclusion, we were unable to detect an increase in initial CPAP adherence by showing patients their actual PSG graphic data. Further studies evaluating the potential role for such intervention are needed in patients with sleep apnea.
Footnotes
- Correspondence: Rashid Nadeem MD, Lovell Federal Health Care Center, 3001 Green Bay Road, North Chicago IL 60064. E-mail: rashid.nadeem{at}va.gov.
The authors have disclosed no conflicts of interest.
Dr Nadeem presented a version of this paper at the 106th International Conference of the American Thoracic Society, held May 14–19, 2010, in New Orleans, Louisiana.
- Copyright © 2013 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}