

Abstract
High-frequency ventilation is commonly utilized with neonates and with children with severe respiratory failure. Both high-frequency oscillatory ventilation (HFOV) and high-frequency jet ventilation (HFJV) are used extensively in neonates. HFJV can also be used in older, larger children. The purpose of this narrative review is to discuss the physiologic principles behind HFJV, examine the evidence supporting its use in neonatal and pediatric ICUs, give meaningful guidance for clinical application, and highlight potential areas for future research.
- high-frequency jet ventilation
- pediatric
- neonate
- mechanical ventilation
- review
- high-frequency jet ventilation
Introduction
Respiratory failure is a common cause of admission to the neonatal ICU or pediatric ICU.1–3 Most infants and children with respiratory failure can be supported using conventional mechanical ventilation; however, those with lower gestational age and more severe respiratory disease may benefit from high-frequency ventilation.4,5 High-frequency oscillatory (HFOV) ventilation and high-frequency jet (HFJV) have been used extensively as lung-protective strategies in premature neonates with severe respiratory failure.5,6 Available data comparing HFOV and HFJV in premature neonates have not shown the superiority of either modality.7 While HFJV use for neonates is relatively common, it has also been successfully used in older infants.8,9
Despite the lack of high-quality evidence, the use of HFJV may be increasing as there have been a number of single-center experiences published since 2015.8–12 The purpose of this review is to discuss the physiologic principles behind HFJV, examine the evidence supporting its use in neonatal and pediatric ICUs, give meaningful guidance for clinical application, and highlight potential areas for future research.
Physiology of Jet Ventilation
High-frequency ventilation has some theoretical advantages over conventional mechanical ventilation, although published literature has shown conflicting results in patient outcomes.13–18 Due to ultrashort inspiratory times (TI), tidal volume (VT) is less than anatomic dead space (1–3 mL/kg) during high-frequency ventilation. This results in a significant attenuation between the pressure at the airway and the pressure at the alveolar level.19 While both HFOV and HFJV share this general principle, there are important differences between modalities. During HFOV, both inhalation and exhalation are active processes controlled by the ventilator.20 Inspiratory to expiration time is usually kept constant at 33%, although this ratio can be changed to affect CO2 clearance. During HFJV, exhalation is passive and dependent upon the rate (ie, cycles or breaths/min), TI, and inspiratory to expiratory (I:E) ratio. Some key differences between HFOV and HFJV are summarized in Table 1.
Differences Between HFOV and HFJV
HFJV delivers high-velocity gas through an electronically activated pinch valve and provides a nearly continuous stream of fresh gas to the alveoli. The resulting PIP is attenuated throughout the respiratory system and theoretically results in a reduction in alveolar pressure.19,21 The HFJV rate can be set between 240 and 660 cycles/min, or 4–11 Hz, with a set TI between 0.02 s and 0.034 s. Increasing the TI results in a larger VT and a reduction in the I-E ratio. To prevent gas-trapping, the HFJV rate may need to be reduced when TI is increased to allow adequate exhalation time. Mean airway pressure ( ) is controlled by a conventional ventilator in tandem with the HFJV ventilator, with PEEP being supplied by the conventional ventilator. During HFJV, PEEP is the primary determinant of
) is controlled by a conventional ventilator in tandem with the HFJV ventilator, with PEEP being supplied by the conventional ventilator. During HFJV, PEEP is the primary determinant of  , and recruitment breaths (also known as the backup rate or sigh breaths) are supplied, generally at a rate of 0–5 breaths/min.
, and recruitment breaths (also known as the backup rate or sigh breaths) are supplied, generally at a rate of 0–5 breaths/min.
HFJV has some theoretical advantages over HFOV due to the flow streaming created by the solenoid pinch valve. The “jet” of gas is inserted into the endotracheal tube via a special adapter (Figure 1). The steady stream of jet pulses down the center of the airway results in a continuous stream of exhaled air up the sides of the airways (Figure 2). This continuous passive exhalation makes HFJV excellent at CO2 elimination, which may be particularly useful for disease processes with impaired ventilation. This can allow for improved ventilation at lower  , an important consideration for patients with air leak or who have hemodynamic compromise from elevated
, an important consideration for patients with air leak or who have hemodynamic compromise from elevated  . Furthermore, the flow streaming of exhaled gas along the walls of the airways theoretically assists with secretion clearance, pushing mucus up and out of the airways.
. Furthermore, the flow streaming of exhaled gas along the walls of the airways theoretically assists with secretion clearance, pushing mucus up and out of the airways.

High-flow jet ventilation endotracheal tube adapter. Courtesy of Bunnell.

Mechanics of gas exchange during high-flow jet ventilation. HFJV = high-frequency jet ventilation; CMV = conventional mechanical ventilation.
Additional advantages of HFJV over HFOV is the pairing of HFJV with a conventional ventilator, which allows for easy assessment of pulmonary mechanics as HFJV can be paused while the patient is ventilated using only the conventional ventilator. Differences in pressure attenuation during HFOV and HFJV are illustrated in Figure 3. This setup also allows rapid transition back and forth between HFJV and conventional ventilator, although it requires 2 ventilators to remain at the bedside. Finally, the HFJV ventilator provides excellent monitoring of airway pressures through the port at the endotracheal tube connector, assisting clinicians in titration of ventilator settings. A significant limitation to HFJV is that the only commercially available jet ventilator can rarely provide the necessary power to ventilate infants above ∼ 10 kg. It is this commercial ventilator from Bunnell (Salt Lake City, Utah) that we will discuss regarding titration of settings.

Comparison of pressure attenuation between high-flow oscillatory ventilation (HFOV) and high-flow jet ventilation (HFJV).
Settings and Technical Considerations
HFJV requires a separate ventilator that is approved by the U.S. Food and Drug Administration for use in neonates ≤ 28 d of age. The conventional mechanical ventilator is used in tandem with the HFJV ventilator and provides PEEP, a set breathing frequency, a set peak inspiratory pressure (PIP), and a set TI. The HFJV ventilator allows separate settings for jet PIP, TI, and breathing frequency (ie, breaths/min).  needs to be set the same on both ventilators.
needs to be set the same on both ventilators.
When initiating HFJV in premature neonates, initial PIP is usually started slightly above (ie, 2–5 cm H2O above) the PIP on the conventional ventilator and adjusted for “appropriate” chest wiggle.12 For patients in the pediatric ICU, the initial PIP may be set in a similar manner, although larger patients may require a high (∼ 40 cm H2O) initial PIP.8,9 Attenuation of the PIP through the large airways and bronchi results in lower pressure in the terminal airways and alveoli. Once initial PIP is determined, it is usually adjusted in increments of 1–2 cm H2O to achieve acceptable  and pH levels. The maximum PIP is 50 cm H2O, a level rarely reached in premature neonates but is commonly required in larger infants or in the pediatric ICU.8 Patients not meeting clinical ventilation targets at a PIP of 50 cm H2O may require transition to HFOV or extracorporeal membrane oxygenation (ECMO), although increasing the TI may also improve ventilation.
and pH levels. The maximum PIP is 50 cm H2O, a level rarely reached in premature neonates but is commonly required in larger infants or in the pediatric ICU.8 Patients not meeting clinical ventilation targets at a PIP of 50 cm H2O may require transition to HFOV or extracorporeal membrane oxygenation (ECMO), although increasing the TI may also improve ventilation.
HFJV rate is usually set based on the patient's size and disease state, with neonates usually initiated at 420 breaths/min.12 In the pediatric ICU, the rate is usually started between 360–420 breaths/min.9 For patients with increased airway resistance, the HFJV rate may need to be reduced further to allow for an increased expiratory time and avoid gas-trapping.8 The HFJV rate is adjusted to prevent intrinsic PEEP, which is usually determined to be present if the PEEP measured by the HFJV ventilator is ≥ 1–2 cm H2O greater than the set PEEP on the conventional ventilator, although this threshold varies between centers.12
Following PIP, TI is the largest determinant of VT, with longer TI delivering larger HFJV VT. TI during HFJV in premature neonates is started at 0.02 s and is rarely increased unless the PIP is high with elevated  levels.12 In larger pediatric patients, a TI of 0.03 s may be used to increase VT but will likely also require a lower HFJV rate to maintain the I-E ratio and prevent intrinsic PEEP due to gas-trapping.8 The majority of patients receiving HFJV do not need to have the TI adjusted during HFJV unless ventilation goals cannot be achieved.
levels.12 In larger pediatric patients, a TI of 0.03 s may be used to increase VT but will likely also require a lower HFJV rate to maintain the I-E ratio and prevent intrinsic PEEP due to gas-trapping.8 The majority of patients receiving HFJV do not need to have the TI adjusted during HFJV unless ventilation goals cannot be achieved.
The conventional ventilator provides PEEP (the primary determinant of  during HFJV) and backup or sigh breaths for lung recruitment, illustrated in Figure 4. The settings used on the conventional ventilator are generally a set breathing frequency of 0–5 breaths/min, PEEP adjusted to the desired
during HFJV) and backup or sigh breaths for lung recruitment, illustrated in Figure 4. The settings used on the conventional ventilator are generally a set breathing frequency of 0–5 breaths/min, PEEP adjusted to the desired  , and PIP set below the HFJV PIP and within the lung-protective range (ie, ≤ 28 cm H2O). As the backup rate is increased, the risk of gas-trapping and intrinsic PEEP also increases. The conventional PIP needs to be kept below the HFJV PIP or the conventional breath will interrupt HFJV delivery. The conventional recruitment or sigh breaths are used to improve oxygenation through lung recruitment if unable to decrease
, and PIP set below the HFJV PIP and within the lung-protective range (ie, ≤ 28 cm H2O). As the backup rate is increased, the risk of gas-trapping and intrinsic PEEP also increases. The conventional PIP needs to be kept below the HFJV PIP or the conventional breath will interrupt HFJV delivery. The conventional recruitment or sigh breaths are used to improve oxygenation through lung recruitment if unable to decrease  or during acute desaturation events.12 In air leak syndromes or in other cases where lung protection is of paramount concern, the ideal lung-protective strategy during HFJV would be a conventional rate set at 0 breaths/min. If unable to decrease the conventional rate, consider increasing the
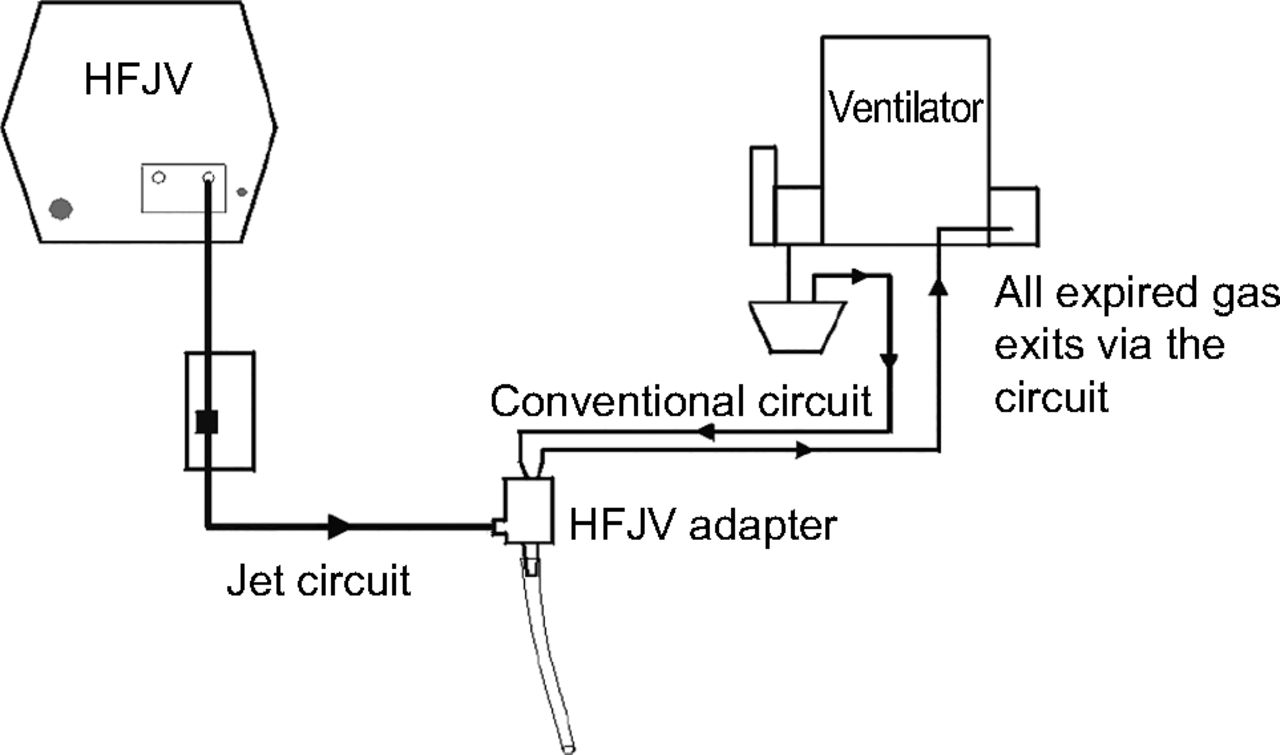
or during acute desaturation events.12 In air leak syndromes or in other cases where lung protection is of paramount concern, the ideal lung-protective strategy during HFJV would be a conventional rate set at 0 breaths/min. If unable to decrease the conventional rate, consider increasing the  by increasing PEEP. There are no published methods to adjust PEEP during HFJV, and it must be done empirically. A schematic of the conventional ventilator and HFJV ventilator is shown in Figure 5.
by increasing PEEP. There are no published methods to adjust PEEP during HFJV, and it must be done empirically. A schematic of the conventional ventilator and HFJV ventilator is shown in Figure 5.

Pressure scalar of high-frequency jet ventilation pressure measured at the patient's airway.

Schematic of conventional ventilator and high-flow jet ventilator (HFJV). Courtesy of Bunnell.
Servo pressure is measured by the HFJV and is displayed on the ventilator and is measured in pressure per square inch (psi). The servo pressure reflects the amount of energy (pressure) the ventilator needs to use to deliver the set PIP. Functionally, if settings are held constant, servo pressure is directly proportional to the amount of lung being ventilated. As such, servo pressure is an important parameter to monitor as changes in servo pressure can indicate changes in lung mechanics, lung recruitment, and patient status. An increase in servo pressure could be related to improved lung compliance, recruitment of atelectatic lung units, decreased airway resistance, increasing leak around the artificial airway, non-tension pneumothorax, or endotracheal tube dislodgement. Conversely, a decrease in servo pressure could be the result of secretions, worsening lung compliance, an increase in airway resistance, tension pneumothorax, endotracheal tube malposition, or obstructed/kinked endotracheal tube. Importantly, servo pressure will also increase or decrease based on the set PIP and delta pressure.
The specialty endotracheal tube adapter can be used with both cuffed and uncuffed endotracheal tubes. The adapter continuously measures  , PEEP, and PIP at the patient's airway. This monitoring capability provides high-quality measurements that can assist clinicians in titrating settings and has been used in bench research due to its accuracy.22 Differences between HFJV use in neonatal ICU versus pediatric ICU are summarized in Table 2.
, PEEP, and PIP at the patient's airway. This monitoring capability provides high-quality measurements that can assist clinicians in titrating settings and has been used in bench research due to its accuracy.22 Differences between HFJV use in neonatal ICU versus pediatric ICU are summarized in Table 2.
Differences Between Neonatal and Pediatric HFJV Management
Studies of HFJV in the Neonatal ICU
Systematic Reviews and Randomized Controlled Trials
HFJV has been used as a rescue mode and as a preemptive strategy in neonates.13 A Cochrane review and meta-analysis of a single study concluded that there was insufficient evidence to support HFJV as a rescue mode in neonates.6 The initial randomized controlled trial (RCT) by Keszler et al,23 performed in 1991, randomized 144 infants ≥ 750 g with pulmonary interstitial emphysema to HFJV or conventional ventilation. The primary outcome was resolution of pulmonary interstitial emphysema. The control group received a PEEP ≤ 5 cm H2O, set rate during intermittent mandatory ventilation of 60–100 breaths/min, and a PIP guided by chest rise and gas exchange. The HFJV group was managed with a PIP 10–20% below the PIP on conventional ventilator. There was no difference in mortality between the groups; however, after excluding those who crossed over from conventional ventilation to HFJV, there was a difference in survival (65% for HFJV vs 47% for conventional ventilation). This benefit was driven by large differences in outcomes for infants weighing 1.0–1.5 kg. HFJV resulted in similar gas exchange with lower  and PIP, yet pulmonary interstitial emphysema resolved faster in the HFJV group.23 This trial provided low-quality evidence as it predates the routine use of surfactant replacement therapy and antenatal steroids, and subjects in the conventional ventilator group received a higher PIP (> 30 cm H2O) than is currently used, as many centers will now consider transition to high-frequency ventilation when the conventional ventilator PIP reaches 25 cm H2O.12
and PIP, yet pulmonary interstitial emphysema resolved faster in the HFJV group.23 This trial provided low-quality evidence as it predates the routine use of surfactant replacement therapy and antenatal steroids, and subjects in the conventional ventilator group received a higher PIP (> 30 cm H2O) than is currently used, as many centers will now consider transition to high-frequency ventilation when the conventional ventilator PIP reaches 25 cm H2O.12
The second study by Keszler et al,24 published in 1997, compared HFJV to conventional ventilation in premature neonates with respiratory distress syndrome.24 Conventional ventilator management was uncontrolled but was generally delivered with a breathing frequency of 30–60 breaths/min and PIP high enough to provide adequate chest rise. Gas exchange targets were pH 7.25–7.40,  35–45 mm Hg, and
35–45 mm Hg, and  50–80 mm Hg. The investigators used an HFJV strategy with PIP equal to the pre-HFJV PIP on conventional ventilation, PEEP 0.5–2 cm H2O above conventional ventilation; other settings were not described. The authors reported reductions in bronchopulmonary dysplasia and need for home oxygen, although there were no differences in survival.24 This trial was significantly limited by protocol deviations and the decision to create different HFJV groups after the trial was completed instead of analyzing outcomes based on intention-to-treat principles. Additionally, this trial was performed prior to the implementation of lung-protective ventilation strategies such as permissive hypercapnia and limiting plateau pressure. In addition, more subjects in the HFJV low group (defined as initiation of HFJV without an increase in set PEEP of ≥ 1 cm H2O) had severe intraventricular hemorrhage or periventricular leukomalacia, while other outcome measures were similar.
50–80 mm Hg. The investigators used an HFJV strategy with PIP equal to the pre-HFJV PIP on conventional ventilation, PEEP 0.5–2 cm H2O above conventional ventilation; other settings were not described. The authors reported reductions in bronchopulmonary dysplasia and need for home oxygen, although there were no differences in survival.24 This trial was significantly limited by protocol deviations and the decision to create different HFJV groups after the trial was completed instead of analyzing outcomes based on intention-to-treat principles. Additionally, this trial was performed prior to the implementation of lung-protective ventilation strategies such as permissive hypercapnia and limiting plateau pressure. In addition, more subjects in the HFJV low group (defined as initiation of HFJV without an increase in set PEEP of ≥ 1 cm H2O) had severe intraventricular hemorrhage or periventricular leukomalacia, while other outcome measures were similar.
Engle et al25 conducted a small RCT (HFJV = 11, conventional ventilation = 13) comparing HFJV to a high-frequency conventional ventilator strategy in infants with persistent pulmonary hypertension. PIP in the conventional ventilator group in this study was 38 cm H2O at baseline and increased to 44 cm H2O 6 h after initiation. There were no statistically significant differences in outcomes between the groups, although the trial was underpowered to detect differences. This trial is not applicable to modern practice as hyperventilation is no longer routinely performed for persistent pulmonary hypertension due to the widespread use of inhaled nitric oxide, although management of persistent pulmonary hypertension usually includes tight control of  .
.
Wiswell et al26 performed an RCT in 73 premature infants > 500 g to HFJV or conventional ventilation. The subjects' mean weight was 881 g, and their gestational age was 26.5 weeks. There were no differences in mortality or development of chronic lung disease, but there were worse neurologic outcomes in the subjects receiving HFJV. Logistic regression confirmed that HFJV was associated with adverse events.26 The poor neurological outcomes in this study were potentially related to decreased cerebral blood flow secondary to hyperventilation experienced during HFJV.
In the 1980s, Carlo et al performed 2 RCTs comparing HFJV to conventional ventilator in premature neonates.27,28 The first trial enrolled 40 subjects with a mean weight of 1.5 kg and 30 weeks gestational age; no differences in major outcomes were reported.27 Subjects on HFJV maintained similar gas exchange despite lower  . A follow-up to this study evaluated tracheobronchial outcomes and concluded that HFJV was not associated with adverse effects.28 The second trial evaluated 42 subjects with a mean weight of 1.4 kg and mean gestational age of 30 weeks; no differences were reported for major outcomes, although
. A follow-up to this study evaluated tracheobronchial outcomes and concluded that HFJV was not associated with adverse effects.28 The second trial evaluated 42 subjects with a mean weight of 1.4 kg and mean gestational age of 30 weeks; no differences were reported for major outcomes, although  and
and  were lower in the subjects receiving HFJV.29 These trials were performed in the 1980s and may not be applicable to modern neonatal ICUs due to changes in mechanical ventilation practices and the routine use of surfactant replacement therapy, antenatal steroids, and noninvasive ventilation.
were lower in the subjects receiving HFJV.29 These trials were performed in the 1980s and may not be applicable to modern neonatal ICUs due to changes in mechanical ventilation practices and the routine use of surfactant replacement therapy, antenatal steroids, and noninvasive ventilation.
Retrospective Studies
Wheeler et al12 evaluated the use of HFJV as rescue ventilation in 53 subjects with significant hypercapnic acidosis (gestational age 25.1 weeks/800 g and 28.4 weeks/1,200 g in survivors and nonsurvivors, respectively). They initiated HFJV when the conventional ventilator PIP was 20 cm H2O in survivors and 21.5 cm H2O in nonsurvivors. HFJV PIP at initiation was 26 cm H2O in survivors and 29 cm H2O in nonsurvivors, and nonsurvivors had a lower pH despite nonsignificantly higher VT (7 vs 8 mL/kg), suggesting that nonsurvivors had higher dead space or increased CO2 production despite similar lung compliance. The survival rate was 74%, and univariate analysis revealed that gender, gestational age, postmenstrual age at HFJV initiation, birth at < 28 weeks gestational age, weight, length of stay, arterial access, inhaled nitric oxide, patent ductus arteriosus,  , PIP at 1 h after HFJV initiation, and oxygen saturation index 4 h after HFJV were all statistically different between survivors and nonsurvivors.12 The survivors in this study were younger, smaller, had lower
, PIP at 1 h after HFJV initiation, and oxygen saturation index 4 h after HFJV were all statistically different between survivors and nonsurvivors.12 The survivors in this study were younger, smaller, had lower  , and higher PEEP at HFJV initiation.
, and higher PEEP at HFJV initiation.
A prior study from the same center evaluated the response to HFJV in a cohort of 34 subjects with significant hypercapnia on conventional ventilation or HFOV.10 Prior to HFJV, median VT was 7 mL/kg and the set breathing frequency was 40 breaths/min; PIP was 19 cm H2O in responders and 25 cm H2O in nonresponders. Response to HFJV was defined as a reduction of ≥ 10% in capillary CO2. The pH values were 7.10 and 7.24 and the capillary CO2 values were 72 and 71 mm Hg in responders and nonresponders, respectively. HFJV was initiated at a PIP of 25 and 26 cm H2O in the 2 groups. Nonresponders had a later postmenstrual age (30 weeks vs 27 weeks) and higher oxygen saturation index (7.25 vs 3.36) at 4 h after initiation.10 Overall survival was 75%, and there was no difference between responders and nonresponders for mortality.
A case-control study involving 50 infants who received HFJV tracked death before discharge or discharge on oxygen as the primary outcomes.11 HFJV was initiated due to pulmonary interstitial emphysema or failure to respond to conventional ventilation or HFOV. Oxygenation failure was defined as  ≥ 10 cm H2O and
≥ 10 cm H2O and  > 0.30 or ventilation failure (
> 0.30 or ventilation failure ( > 45 mm Hg and pH < 7.20) with a VT of 4–6 mL/kg. HFJV was initiated at a rate of 240 breaths/min. HFJV was associated with higher incidence of death before discharge or home oxygen and longer duration of mechanical ventilation, although subjects on HFJV were less likely to require treatment for retinopathy of prematurity.11 The subjects on HFJV were likely to be sicker as they had a higher
> 45 mm Hg and pH < 7.20) with a VT of 4–6 mL/kg. HFJV was initiated at a rate of 240 breaths/min. HFJV was associated with higher incidence of death before discharge or home oxygen and longer duration of mechanical ventilation, although subjects on HFJV were less likely to require treatment for retinopathy of prematurity.11 The subjects on HFJV were likely to be sicker as they had a higher  and
and  , but they were less likely to receive diuretics and adjuvant therapies. Another study evaluated HFJV in 6 infants with air leak, and HFJV was associated with a significant decrease in air leak through chest tubes.30 Subjects on HFJV received much lower PIP (28 vs 41 cm H2O) and
, but they were less likely to receive diuretics and adjuvant therapies. Another study evaluated HFJV in 6 infants with air leak, and HFJV was associated with a significant decrease in air leak through chest tubes.30 Subjects on HFJV received much lower PIP (28 vs 41 cm H2O) and  (15.0 vs 9.7 cm H2O) in this study, so it is unclear if the reduction in air leak was related to HFJV or the reduction in airway pressures.
(15.0 vs 9.7 cm H2O) in this study, so it is unclear if the reduction in air leak was related to HFJV or the reduction in airway pressures.
Noonan et al31 compared outcomes between HFJV (n = 23) and conventional ventilator (n = 25) for patent ductus arteriosus closure in neonates via thoracotomy. Conventional ventilator subjects were younger but were otherwise similar to subjects in the HFJV group, although  was slightly higher in the HFJV group (11 vs 10 cm H2O, P = .056). Following patent ductus arteriosus closure, CO2 levels were lower in subjects treated with HFJV, but no other differences were noted 24 h and 7 d after closure. No surgical morbidity differences were noted between the 2 groups.31 This study demonstrated that subjects do not need to be removed from HFJV to perform patent ductus arteriosus closure.
was slightly higher in the HFJV group (11 vs 10 cm H2O, P = .056). Following patent ductus arteriosus closure, CO2 levels were lower in subjects treated with HFJV, but no other differences were noted 24 h and 7 d after closure. No surgical morbidity differences were noted between the 2 groups.31 This study demonstrated that subjects do not need to be removed from HFJV to perform patent ductus arteriosus closure.
The use of HFJV was evaluated in a cohort of 16 subjects with congenital diaphragmatic hernia. Survival in the HFJV cohort was higher than predicted; however, this was limited by the small sample size.32 Another center reported their experience using HFJV in 25 infants with congenital diaphragmatic hernia with improved ventilation, including general ventilation guidelines:  < 12 cm H2O, PIP ≤ 25 cm H2O, mild-moderate permissive hypercapnia (pH > 7.25), and target
< 12 cm H2O, PIP ≤ 25 cm H2O, mild-moderate permissive hypercapnia (pH > 7.25), and target  ≥ 85%; the authors did not report the specific settings used. The mortality rate was 64%.33 Importantly, congenital diaphragmatic hernia may be managed in both neonatal ICUs and pediatric ICUs, depending on the center.32,33
≥ 85%; the authors did not report the specific settings used. The mortality rate was 64%.33 Importantly, congenital diaphragmatic hernia may be managed in both neonatal ICUs and pediatric ICUs, depending on the center.32,33
Coates et al34 compared outcomes between infants with persistent pulmonary hypertension treated with HFJV (n = 22) and HFOV (n = 43). Subjects treated with HFJV were less likely to need ECMO, although the HFOV group was sicker at baseline. After adjustment for baseline differences, the authors concluded there was no difference between groups in terms of risk for ECMO. Importantly, a separate study reported that HFJV does not affect response to inhaled nitric oxide.35
The use of HFJV during inter-hospital transport was found to be safe and associated with decreased  in subjects treated with HFJV, although it had no effect on oxygenation.36 Importantly,
in subjects treated with HFJV, although it had no effect on oxygenation.36 Importantly,  was < 35 mm Hg on average in subjects treated with HFJV, which has important implications as hypocapnia has been associated with worse neurological status in neonates.
was < 35 mm Hg on average in subjects treated with HFJV, which has important implications as hypocapnia has been associated with worse neurological status in neonates.
Plavka et al37 initiated HFJV in 10 infants with worsening lung disease on conventional ventilation. HFJV was initiated when a VT ≥ 7 mL/kg with adequate PEEP was unable to maintain  < 60 mm Hg or the oxygenation index was > 10 and increasing. HFJV rate was set between 310 and 420 breaths/min, with a median PIP of 23 cm H2O. The authors reported a decrease in
< 60 mm Hg or the oxygenation index was > 10 and increasing. HFJV rate was set between 310 and 420 breaths/min, with a median PIP of 23 cm H2O. The authors reported a decrease in  and oxygenation index over time, and 90% survived to hospital discharge, although all 9 survivors were diagnosed with chronic lung disease. A separate study evaluated the effect of transitioning from HFOV to HFJV in 10 subjects with refractory hypoxemia related to worsening chronic lung disease and pneumonia.38 The oxygenation index decreased from 29 to 18 at 3 h after transition to HFJV, and survival was 90%.38 A different study concluded that hypocapnia related to HFJV was associated with periventricular leukomalacia in premature neonates and was significantly related to a
and oxygenation index over time, and 90% survived to hospital discharge, although all 9 survivors were diagnosed with chronic lung disease. A separate study evaluated the effect of transitioning from HFOV to HFJV in 10 subjects with refractory hypoxemia related to worsening chronic lung disease and pneumonia.38 The oxygenation index decreased from 29 to 18 at 3 h after transition to HFJV, and survival was 90%.38 A different study concluded that hypocapnia related to HFJV was associated with periventricular leukomalacia in premature neonates and was significantly related to a  < 25 mm Hg in the first 3 d of life.39 Another single-center study evaluated subjects transferred to their facility for potential ECMO and divided them into HFJV responders to nonresponders who required ECMO.40 Oxygenation index significantly decreased in both groups but remained high in the nonresponders.40 Importantly, this study was performed prior to the availability of inhaled nitric oxide.
< 25 mm Hg in the first 3 d of life.39 Another single-center study evaluated subjects transferred to their facility for potential ECMO and divided them into HFJV responders to nonresponders who required ECMO.40 Oxygenation index significantly decreased in both groups but remained high in the nonresponders.40 Importantly, this study was performed prior to the availability of inhaled nitric oxide.
Animal Studies in Neonatal Models
HFJV was compared to low volume conventional ventilation in a neonatal lung injury/meconium aspiration rabbit model over 4 h.41 The conventional ventilator was reported to be superior at 1 h, but no other differences were noted. HFJV was compared to synchronized intermittent mandatory ventilation in preterm lambs where the conventional ventilator group received VT of 5 mL/kg for 5 min and then VT was increased to 7 mL/kg with a maximum PIP of 40 cm H2O and a PEEP of 7 cm H2O.  was targeted at 45–55 mm Hg.42 HFJV was initiated at a rate of 420 breaths/min, PIP of 40 cm H2O, and PEEP of 8 cm H2O, and permissive hypercapnia was allowed. The authors did not report any major differences between groups, including inflammatory markers and postmortem examination.42 Importantly, they did not report the PIP received by the control arm in this study.
was targeted at 45–55 mm Hg.42 HFJV was initiated at a rate of 420 breaths/min, PIP of 40 cm H2O, and PEEP of 8 cm H2O, and permissive hypercapnia was allowed. The authors did not report any major differences between groups, including inflammatory markers and postmortem examination.42 Importantly, they did not report the PIP received by the control arm in this study.
Three different methods and 2 catheter sizes used during closed suctioning with HFJV were evaluated in rabbits. The authors compared suctioning with HFJV running, HFJV paused, and suctioning while inserting and removing the catheter. No differences were reported for lung volumes between groups, and lung volumes recovered within 60 s for all groups. There were greater differences for 8 French catheters, but lung volume was restored after 3 recruitment breaths.43 Musk et al44 evaluated the effect of increasing TI during conventional breaths from 0.5 s to 2 s during HFJV in preterm lambs; no differences in oxygenation between groups were reported, although there were increased inflammatory markers in the group with the longer TI. In a rabbit model of meconium aspiration syndrome, HFJV was not more effective than suctioning during conventional ventilation, although HFJV did result in slight improvements in gas exchange.45
Recommendations for Clinical Practice
HFJV is used as both a rescue mode in severely ill patients and as a prophylactic treatment in extremely low birthweight infants at high risk of developing bronchopulmonary dysplasia or chronic lung disease. In infants born at < 26 weeks gestation, HFJV may be considered upon admission to the neonatal ICU without a trial of conventional ventilation. The fragile premature lung in the early phases of lung development could theoretically be protected by providing more “gentle” ventilation with HFJV. The premature lung is susceptible to lung injury as there are varying degrees of lung development that are dependent upon the patient's gestational age. While many premature infants have minimal lung disease at birth, bronchopulmonary dysplasia remains a common complication resulting in significant morbidity and mortality.
Premature infants with respiratory distress syndrome may be also placed on the HFJV if surfactant administration and conventional ventilator have not achieved adequate gas exchange or ventilator support exceeds predetermined thresholds. A set breathing frequency of 40 breaths/min and PIP > 23 cm H2O are the thresholds used in our center to initiate HFJV.
In infants with air leak (eg, pneumothorax or pulmonary interstitial emphysema), HFJV can be used to allow the lung to heal.23,30 Due to pressure attenuation during HFJV, it may be more protective than conventional ventilation. For infants with air leak, permissive hypercapnia should be utilized, and HFJV PIP and  should be kept at the minimum levels to allow adequate gas exchange (pH > 7.20–7.25,
should be kept at the minimum levels to allow adequate gas exchange (pH > 7.20–7.25,  > 85%). The HFJV breathing frequency should be initiated at 420 breaths/min, and TI should not exceed 0.02 s. The backup rate on the conventional ventilator should be set as low as possible, with a goal of 0 breaths/min. In pulmonary interstitial emphysema patients, special care should be taken when chest radiographs demonstrate hyperinflation. The general response to hyperinflation is to decrease
> 85%). The HFJV breathing frequency should be initiated at 420 breaths/min, and TI should not exceed 0.02 s. The backup rate on the conventional ventilator should be set as low as possible, with a goal of 0 breaths/min. In pulmonary interstitial emphysema patients, special care should be taken when chest radiographs demonstrate hyperinflation. The general response to hyperinflation is to decrease  by decreasing PEEP, but oxygenation may worsen. These patients are usually on moderate PEEP settings of 4–6 cm H2O and intermittent mandatory ventilation rates ≤ 5 breaths/min. To allow a low conventional ventilation rate, PEEP may need to be increased 2–3 cm H2O. Airway structures that are not adequately supported can partially or fully collapse, causing air-trapping. The PIP set on the conventional ventilator should be 4–5 cm H2O below the HFJV PIP.
by decreasing PEEP, but oxygenation may worsen. These patients are usually on moderate PEEP settings of 4–6 cm H2O and intermittent mandatory ventilation rates ≤ 5 breaths/min. To allow a low conventional ventilation rate, PEEP may need to be increased 2–3 cm H2O. Airway structures that are not adequately supported can partially or fully collapse, causing air-trapping. The PIP set on the conventional ventilator should be 4–5 cm H2O below the HFJV PIP.
Infants with congenital diaphragmatic hernia, meconium aspiration, or persistent pulmonary hypertension may also benefit from HFJV. Gas streaming during HFJV may be helpful in secretion removal in infants with meconium aspiration, although studies on the effect of HFJV on secretion removal have not been performed. HFJV has some theoretic benefits when compared to HFOV in this patient population as passive exhalation and ability to adjust the I:E ratio may result in improved gas exchange in patients with high airway resistance or lung unit with differing time constants. In infants with congenital diaphragmatic hernia and persistent pulmonary hypertension, HFJV can provide ventilation with lower pressures than a conventional ventilator. Due to their larger size, term infants with congenital diaphragmatic hernia or meconium aspiration may require a lower HFJV rate or an increase in TI.
Conventional ventilator settings will vary based on the underlying lung disease. In infants with reduced lung compliance due to respiratory distress syndrome, pneumonia, or meconium aspiration syndrome, conventional ventilator settings would typically include a backup breathing frequency of 3–5 breaths/min. This is intended to provide ongoing lung recruitment, although the conventional rate should be minimized to avoid ventilator-induced lung injury. If there is a difference of ≥ 1–2 cm H2O between set and PEEP measured by the HFJV ventilator, air-trapping is likely and the conventional rate should be reduced. Other strategies to reduce air-trapping include decreasing the HFJV rate by 60 breaths/min and re-evaluating over 10–15 min.
Initial PEEP should be 5–8 cm H2O. If underexpansion and atelectasis are noted on chest radiograph, the PEEP level may need to be increased. If  cannot be decreased or continues to increase, or if the infant needs frequent interventions for desaturation episodes, the
cannot be decreased or continues to increase, or if the infant needs frequent interventions for desaturation episodes, the  will also likely need to be increased by increasing PEEP. The
will also likely need to be increased by increasing PEEP. The  may be excessive if there is a decreased cardiac silhouette or hemodynamic instability. If hyperinflation is present on chest radiograph, consider decreasing the backup rate on the conventional ventilator or HFJV rate as air-trapping may be related to small airway collapse. PEEP is generally adjusted in increments of 1–2 cm H2O.
may be excessive if there is a decreased cardiac silhouette or hemodynamic instability. If hyperinflation is present on chest radiograph, consider decreasing the backup rate on the conventional ventilator or HFJV rate as air-trapping may be related to small airway collapse. PEEP is generally adjusted in increments of 1–2 cm H2O.
As patients on HFJV improve, the HFJV PIP is gradually reduced in increments of 1–2 cm H2O until they are ready to transition from HFJV to conventional ventilation. There are 2 strategies for weaning from HFJV. The first is to wean and extubate directly from HFJV, usually to noninvasive ventilation or high-flow nasal cannula. This option is more common in infants who have recovered from air leak syndromes. Extubation from HFJV can be considered when HFJV PIP is ≤ 20 cm H2O. The HFJV rate can also be weaned as low as 240 breaths/min if there is still some uncertainty regarding extubation readiness.
No studies have specifically evaluated when to transition back to conventional ventilation. The infant may also be transitioned back to conventional ventilation and then weaned to extubation. In this case, it is recommended to transition when  is ≤ 8–10 cm H2O. Conventional ventilator settings after the transition should include a set breathing frequency < 35 breaths/min, PIP ≤ 20 cm H2O, and PEEP of 5–8 cm H2O. Patients should be extubated as soon as possible after transition, and some patients may only require a few hours of conventional ventilation prior to extubation.
is ≤ 8–10 cm H2O. Conventional ventilator settings after the transition should include a set breathing frequency < 35 breaths/min, PIP ≤ 20 cm H2O, and PEEP of 5–8 cm H2O. Patients should be extubated as soon as possible after transition, and some patients may only require a few hours of conventional ventilation prior to extubation.
Summary of HFJV in the Neonatal ICU
HFJV is indicated for pulmonary interstitial emphysema or air leak syndrome in neonates. The use of preemptive HFJV to prevent perinatal lung disease is not supported by data from RCTs. HFJV can also be considered as a rescue mode in patients with poor lung compliance, in infants with congenital diaphragmatic hernia, and in those with refractory hypercapnia. HFJV's effect on oxygenation in premature and term neonates is unclear, as some studies have shown improved oxygenation while others have shown minimal effect, although this is confounded by differing methods used to set the  .
.
Studies of HFJV in the Pediatric ICU
Clinical Studies in the Pediatric ICU
The use of HFJV in the pediatric ICU has been limited to small, single-center case series. The use of HFJV as a rescue modality was recently investigated in a quaternary pediatric ICU in a retrospective study of 35 infants (median age 2.9 months and weight 5.2 kg) with multiple etiologies of respiratory failure. HFJV improved CO2 clearance but had no effect on oxygenation. In this study, 29% of subjects failed HFJV within 4–6 h of initiation, and 43% required other high-frequency modes or ECMO. The median initial HFJV PIP was 46 cm H2O with a rate of 360 breaths/min and  of 14 cm H2O. ECMO was required for 26% of subjects, and the overall survival was 74%.8 They also found that nonsurvivors were less likely to have a documented infection and had lower scores on the Pediatric Index of Mortality 2; nonsurvivors also had lower pH, HCO3, and base deficit values, but these differences were not statistically significant, suggesting a metabolic component to the acidosis.
of 14 cm H2O. ECMO was required for 26% of subjects, and the overall survival was 74%.8 They also found that nonsurvivors were less likely to have a documented infection and had lower scores on the Pediatric Index of Mortality 2; nonsurvivors also had lower pH, HCO3, and base deficit values, but these differences were not statistically significant, suggesting a metabolic component to the acidosis.
Respiratory syncytial virus and other respiratory viruses can cause critical bronchiolitis or pediatric ARDS. The use of HFJV in children with respiratory syncytial virus who failed conventional ventilation was described in a case series of 12 infants with weights ranging from 1.7 to 14.2 kg. Subjects required HFJV primarily due to hypercapnia, although 11 of 12 subjects met criteria for pediatric ARDS. The survival rate was 91%. HFJV improved ventilation, but there was no significant change in oxygenation index over time.9 Importantly, the HFJV settings used, initiation criteria, and detailed data prior to HFJV initiation were not reported.
In a case report in an infant with barotrauma and severe hypercapnia, HFJV was used with a helium-oxygen mixture as the driving gas during HFJV, resulting in improved  levels.46 In this report, the subject had a low
levels.46 In this report, the subject had a low  requirement and the setup used would not have allowed for oxygen adjustment as the HFJV blender was replaced with the helium-oxygen mixture.
requirement and the setup used would not have allowed for oxygen adjustment as the HFJV blender was replaced with the helium-oxygen mixture.
HFJV was evaluated in 29 subjects with pediatric ARDS and air leak syndrome (mean age 1.0 ± 1.2 y). The survival rate was 69%. Prior to HFJV, conventional ventilator PIP was 48 cm H2O and  was 45 mm Hg.47 This study predates the widespread adoption of lung-protective ventilation and permissive hypercapnia and indicates that HFJV may have some utility in treating air leak syndrome.
was 45 mm Hg.47 This study predates the widespread adoption of lung-protective ventilation and permissive hypercapnia and indicates that HFJV may have some utility in treating air leak syndrome.
Several studies have evaluated the effect of HFJV on gas exchange and hemodynamics in infants and children with congenital heart disease. These have been small, single-center studies from the early 1990s with limited applicability in current pediatric ICUs. HFJV used was evaluated prospectively in 9 subjects (mean age 9 months; weight was not reported) after congenital heart surgery who met pulmonary criteria for ECMO. ECMO criteria were met predominantly due to pulmonary hypertension. Ventilation and oxygenation improved during HFJV with similar PIP and  as during conventional ventilation with stable hemodynamics. ECMO was avoided in all but 1 subject. The mortality rate was 33%, and one subject developed a pneumothorax.48 Thirteen subjects between 0.9 y and 8.5 y old (mean age 3.9 y, mean weight 13.9 kg) were studied after Fontan operation.49 In these subjects with passive pulmonary blood flow, ventilation was achieved with a lower
as during conventional ventilation with stable hemodynamics. ECMO was avoided in all but 1 subject. The mortality rate was 33%, and one subject developed a pneumothorax.48 Thirteen subjects between 0.9 y and 8.5 y old (mean age 3.9 y, mean weight 13.9 kg) were studied after Fontan operation.49 In these subjects with passive pulmonary blood flow, ventilation was achieved with a lower  (9 vs 5 cm H2O), although there were no differences in
(9 vs 5 cm H2O), although there were no differences in  . Improved hemodynamics were observed, likely due to the reduction in
. Improved hemodynamics were observed, likely due to the reduction in  . Cardiac index increased during HFJV and then returned to baseline.49 Current management after the Fontan procedure is early extubation and avoidance of positive-pressure ventilation; it is unclear if HFJV still has a role in the management of children after the Fontan procedure as current devices may not be able to ventilate larger children effectively.
. Cardiac index increased during HFJV and then returned to baseline.49 Current management after the Fontan procedure is early extubation and avoidance of positive-pressure ventilation; it is unclear if HFJV still has a role in the management of children after the Fontan procedure as current devices may not be able to ventilate larger children effectively.
Vincent et al50 studied six infants (mean age 3.5 months, weight 2.4–5.7 kg) receiving HFJV after cardiac surgery were evaluated. Ventilation was achieved with lower PIP, significantly lower tracheal pressure (24 vs 14 cm H2O) with no change in measured hemodynamic parameters.50 A similar study of 6 infants after cardiac surgery demonstrated a significant decrease in PIP from 25 cm H2O to 11 cm H2O and reduction in  from 7 cm H2O to 5 cm H2O, although the decrease in
from 7 cm H2O to 5 cm H2O, although the decrease in  was related to the decrease in set PEEP. The authors reported no relationship between HFJV and cardiac index, although HFJV resulted in a 33% increase in patients with low cardiac index.51 These studies indicate that HFJV may have a role to play in patients with right-ventricular failure or passive pulmonary blood flow, although more data are needed.
was related to the decrease in set PEEP. The authors reported no relationship between HFJV and cardiac index, although HFJV resulted in a 33% increase in patients with low cardiac index.51 These studies indicate that HFJV may have a role to play in patients with right-ventricular failure or passive pulmonary blood flow, although more data are needed.
Animal Studies of HFJV
Various animal models have evaluated HFJV. Airway pressure and gas exchange were compared between conventional ventilator, HFJV, and HFOV in 12 pigs weighing 10–16 kg.52 HFJV resulted in improved ventilation and higher cardiac index with a lower  . In this study,
. In this study,  measured at the airway and the trachea were nearly identical. This is in contrast to a human study in which tracheal pressure was significantly lower.50 This study examined HFJV in a configuration that may not be used in clinical practice in pediatric ICUs because the HFJV ventilator used is not commercially available and the animals receiving conventional ventilation did not receive lung protective ventilation. In addition, the HFJV rate was set at 150 breaths/min with an I:E ratio of 1:2, settings that are not possible on currently available HFJV ventilators. Another study evaluated the
measured at the airway and the trachea were nearly identical. This is in contrast to a human study in which tracheal pressure was significantly lower.50 This study examined HFJV in a configuration that may not be used in clinical practice in pediatric ICUs because the HFJV ventilator used is not commercially available and the animals receiving conventional ventilation did not receive lung protective ventilation. In addition, the HFJV rate was set at 150 breaths/min with an I:E ratio of 1:2, settings that are not possible on currently available HFJV ventilators. Another study evaluated the  measured at the airway compared with the mean alveolar pressures in rabbits weighing between 3.0 kg and 3.95 kg. In this study,
measured at the airway compared with the mean alveolar pressures in rabbits weighing between 3.0 kg and 3.95 kg. In this study,  accurately estimated mean alveolar pressure during HFJV when the rate was between 300 and 600 breath/min.53 HFJV was compared to HFOV in cats with a mean weight of 4.5 kg, and HFJV resulted in lower
accurately estimated mean alveolar pressure during HFJV when the rate was between 300 and 600 breath/min.53 HFJV was compared to HFOV in cats with a mean weight of 4.5 kg, and HFJV resulted in lower  and higher pH with similar airway pressures but no change in oxygenation. Transition from HFJV to HFOV resulted in acidosis, increased pulmonary artery pressure, increased pulmonary vascular resistance, and a decrease in cardiac output.54
and higher pH with similar airway pressures but no change in oxygenation. Transition from HFJV to HFOV resulted in acidosis, increased pulmonary artery pressure, increased pulmonary vascular resistance, and a decrease in cardiac output.54
Bench Studies of HFJV
Aerosol delivery during HFJV was evaluated using magnetic resonance imaging of a phantom lung. Aerosol delivery was lower during HFJV than HFOV, but both were lower than during conventional ventilation.55 Importantly, this study utilized the MiniHeart nebulizer (WestMed Inc, Tucson, Arizona) driven by 2 L/min of flow within the inspiratory limb of the ventilator circuit. Another study evaluated a mathematical equation to predict the PEEP setting needed to match the  when transitioning between HFJV and HFOV; the equation predicted the set PEEP within 0.3 cm H2O.22 The authors also suggest that, when initiating HFJV, clinicians should increase the
when transitioning between HFJV and HFOV; the equation predicted the set PEEP within 0.3 cm H2O.22 The authors also suggest that, when initiating HFJV, clinicians should increase the  by 4–6 cm H2O as is done when initiating HFOV. A separate bench model demonstrated that inhaled nitric oxide can be delivered safely and reliably during HFJV.56
by 4–6 cm H2O as is done when initiating HFOV. A separate bench model demonstrated that inhaled nitric oxide can be delivered safely and reliably during HFJV.56
Recommendations for Clinical Practice
Based on available data from case series, HFJV can be considered as a rescue mode for patients with hypercapnic respiratory failure resulting from acute viral infection.8,9 Available data do not suggest that HFJV improves oxygenation, thus its utility in treating pediatric ARDS may be limited. If initiating HFJV for pediatric ARDS, we suggest increasing the  by 2–5 cm H2O during initiation. In postoperative cardiac patients, HFJV could be considered as a rescue mode for severe hypercapnia or as a strategy to reduce
by 2–5 cm H2O during initiation. In postoperative cardiac patients, HFJV could be considered as a rescue mode for severe hypercapnia or as a strategy to reduce  in patients with passive pulmonary blood flow. Current commercially available HFJV ventilators have a weight limit of ∼ 10 kg.
in patients with passive pulmonary blood flow. Current commercially available HFJV ventilators have a weight limit of ∼ 10 kg.
In patients with increased airway resistance, such as those with bronchiolitis, the HFJV rate should be started at 360 breaths/min and adjusted for air-trapping, as measured by the difference between set PEEP and PEEP measured by the HFJV ventilator. In larger patients, consider increasing the TI to increase the VT if ventilation is inadequate. For patients with poor oxygenation, increasing the  by increasing PEEP or increasing the frequency of sigh breaths may increase lung recruitment. Given concerns for gas-trapping and lung stress, we do not recommend increasing the TI for backup breaths to improve lung recruitment.44
by increasing PEEP or increasing the frequency of sigh breaths may increase lung recruitment. Given concerns for gas-trapping and lung stress, we do not recommend increasing the TI for backup breaths to improve lung recruitment.44
There is little data suggesting when to transition back to conventional ventilation, with one study reporting the successful transition to conventional ventilation when subjects were receiving an HFJV PIP of 39 cm H2O at the time of transition.8 In light of the lack of data, we recommend daily discussion about assessing the patient's pulmonary mechanics. This can easily be accomplished by pausing the HFJV ventilator and increasing the conventional ventilator rate. While this is not standard practice, daily assessments could be made to evaluate trends in pulmonary mechanics over time. Another strategy we have used at our center is to provide manual ventilation with a pneumotachograph inline, although we prefer to evaluate mechanics using the mechanical ventilator.
Summary of HFJV in the Pediatric ICU
There is a paucity of data evaluating HFJV in the pediatric ICU, and most studies have been small, single-center case series or physiologic studies without control groups. HFJV may have utility in refractory hypercapnia due to viral bronchiolitis or air leak syndrome and after cardiac surgery to reduce  to optimize hemodynamics, although the impact on outcomes for any of these populations requires further investigation. Studies have not shown improvement in oxygenation after HFJV initiation. There are a variety of potential uses for HFJV in the pediatric patient; however, they require rigorous investigation in RCTs to fully understand the impact of HFJV.
to optimize hemodynamics, although the impact on outcomes for any of these populations requires further investigation. Studies have not shown improvement in oxygenation after HFJV initiation. There are a variety of potential uses for HFJV in the pediatric patient; however, they require rigorous investigation in RCTs to fully understand the impact of HFJV.
Summary and Future Directions
Future research of HFJV in neonates should include large, multicenter RCTs comparing HFJV as a rescue or lung-protective preventive modality in premature neonates. Prospective observational studies should also be considered to rigorously investigate methods to set  and monitor interactions between the conventional ventilator and HFJV. In particular, when to transition from HFJV to conventional ventilation is an area where data are lacking. Outcomes of these studies should focus not only on survival and the development of chronic lung disease but also consider survival without disability as an outcome. This will require longer follow-up to evaluate survivors for longer-term neurodevelopment outcomes.
and monitor interactions between the conventional ventilator and HFJV. In particular, when to transition from HFJV to conventional ventilation is an area where data are lacking. Outcomes of these studies should focus not only on survival and the development of chronic lung disease but also consider survival without disability as an outcome. This will require longer follow-up to evaluate survivors for longer-term neurodevelopment outcomes.
In the pediatric ICU, HFJV use is rare, used primarily as a rescue mode. As such, any future RCTs would be challenging to perform because refractory respiratory failure is relatively rare and centers with the expertise to use HFJV in these patients are limited. HFJV could be investigated in prospective physiologic studies using electric impedance tomography to measure lung volumes and methods to set  . As with neonatal HFJV, further studies on when to transition to conventional ventilation are needed. A large, multicenter observational trial of rescue modes to increase sample sizes and enable advanced statistical techniques may help us gain insight into the utility of HFJV in the pediatric ICU compared to other rescue modalities.
. As with neonatal HFJV, further studies on when to transition to conventional ventilation are needed. A large, multicenter observational trial of rescue modes to increase sample sizes and enable advanced statistical techniques may help us gain insight into the utility of HFJV in the pediatric ICU compared to other rescue modalities.
HFJV has been used in a variety of patient populations, although high-quality evidence of benefit is lacking. HFJV can be considered for premature neonates with respiratory distress syndrome, as a rescue mode for neonates failing conventional mechanical ventilation, and in patients with hypercapnic respiratory failure in the pediatric ICU.
Footnotes
- Correspondence: Andrew G Miller MSc RRT RRT-ACCS RRT-NPS FAARC, Duke University Medical Center, 2301 Erwin Rd, Durham, NC 27710. E-mail: andrew.g.miller{at}duke.edu
Mr Miller has disclosed a relationship with Ventec Life Systems. Ms Bartle and Dr Rehder have disclosed no conflicts of interest.
- Copyright © 2021 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}