

Abstract
The exponential increase in the complexity of ventilator technology has created a growing knowledge gap that hinders education, research, and ultimately the quality of patient care. This gap is best addressed with a standardized approach to educating clinicians, just as education for basic and advanced life support classes is standardized. We have developed such a program, called Standardized Education for Ventilatory Assistance (SEVA), based on a formal taxonomy for modes of mechanical ventilation. The SEVA program is a progressive system of 6 sequential courses starting from an assumption of no prior knowledge and proceeding to full mastery of advanced techniques. The vision of the program is to provide a unique platform for standardizing training by unifying the concepts of physics, physiology, and technology of mechanical ventilation. The mission is to use both online and in-person simulation-based instruction that has both self-directed and instructor-led components to elevate the skills of health care providers to the mastery level. The first 3 levels of SEVA are free and open to the public. We are developing mechanisms to offer the other levels. Spinoffs of the SEVA program include a free smartphone app that classifies virtually all modes on all ventilators used in the United States (Ventilator Mode Map), a free biweekly online training sessions focusing on waveform interpretation (SEVA-VentRounds), and modifications to the electronic health care record system for entering and charting ventilator orders.
. . . let us go down, and there confound their language, that they may not understand one another’s speech.
Genesis 11:8 King James Version of the Holy Bible
Introduction
I am deeply honored to deliver the second Robert M Kacmarek Scientific Memorial Lecture (Fig. 1). Bob was my friend and colleague. I worked with him at medical conferences all over the world, from Mexico to South America, Japan, and across the United States. I consider Bob to be the most influential respiratory therapist (RT) in the history of our profession. He was an exemplar in clinical practice, research, and especially education. In fact, I first met Bob back in the late 1970s when he was giving seminars on how to take the very first clinical simulation test for the National Board for Respiratory Care Registry exam. A quick search in PubMed will demonstrate that Bob published more research articles than any other RT. In addition, he is the author of several textbooks. Perhaps most notably, he was one of the editors of Egan’s Fundamentals of Respiratory Care.

Tribute to Bob Kacmarek PhD RRT FAARC.
To begin with, it is important to note that as far back as 2007 Bob was part of an American Association for Respiratory Care (AARC) task force to envision the RT of the future. Bob was the lead author on a paper describing the task force published in Respiratory Care in 2009.1 As the paper states, the goal was to identify potential new roles and responsibilities of RTs in 2015 and beyond. But more importantly for this talk, Bob followed up with a paper describing his vision of the competencies of future RTs in the area of mechanical ventilation.2 Specifically, he said that RTs must be technical experts on every aspect of the mechanical ventilator, able to compare capabilities of ventilators, be skilled in ventilator waveform analysis, and most importantly, must know, in detail, the action of all modes and adjuncts. Unfortunately, Bob’s paper provided no guidance in how to achieve these lofty goals, hence the motivation for this paper.
Let’s start with a consideration of how advances in ventilator technology have created a huge educational problem. Back when I was in school (in the last century), the very first book I used on the topic of respiratory care equipment3 mentioned only 3 modes of ventilation. Indeed, only a few ventilators (like the Bourns LS 104–150 infant ventilator) had knobs with mode labels. Nobody gave any thought to what names were used to identify modes, and that attitude has continued to the present. Fast forward to today. The most recent equipment book4 lists almost 500 unique names for modes on 55 different ventilators. It is not uncommon for ICU ventilators to have dozens of modes. (Indeed, on one ventilator I have documented 75 different names for modes, whereas the operator’s manual only identifies 16.) And yet there are certainly not over 500 modes that are actually distinct according to a formal classification scheme. In this textbook, which classifies all modes on all ventilators according to a formal taxonomy, there are only 74 unique modes. A taxonomy is a classification system. I intend to convince the reader that mode classification is the first step in bridging the knowledge gap created by advanced technology.
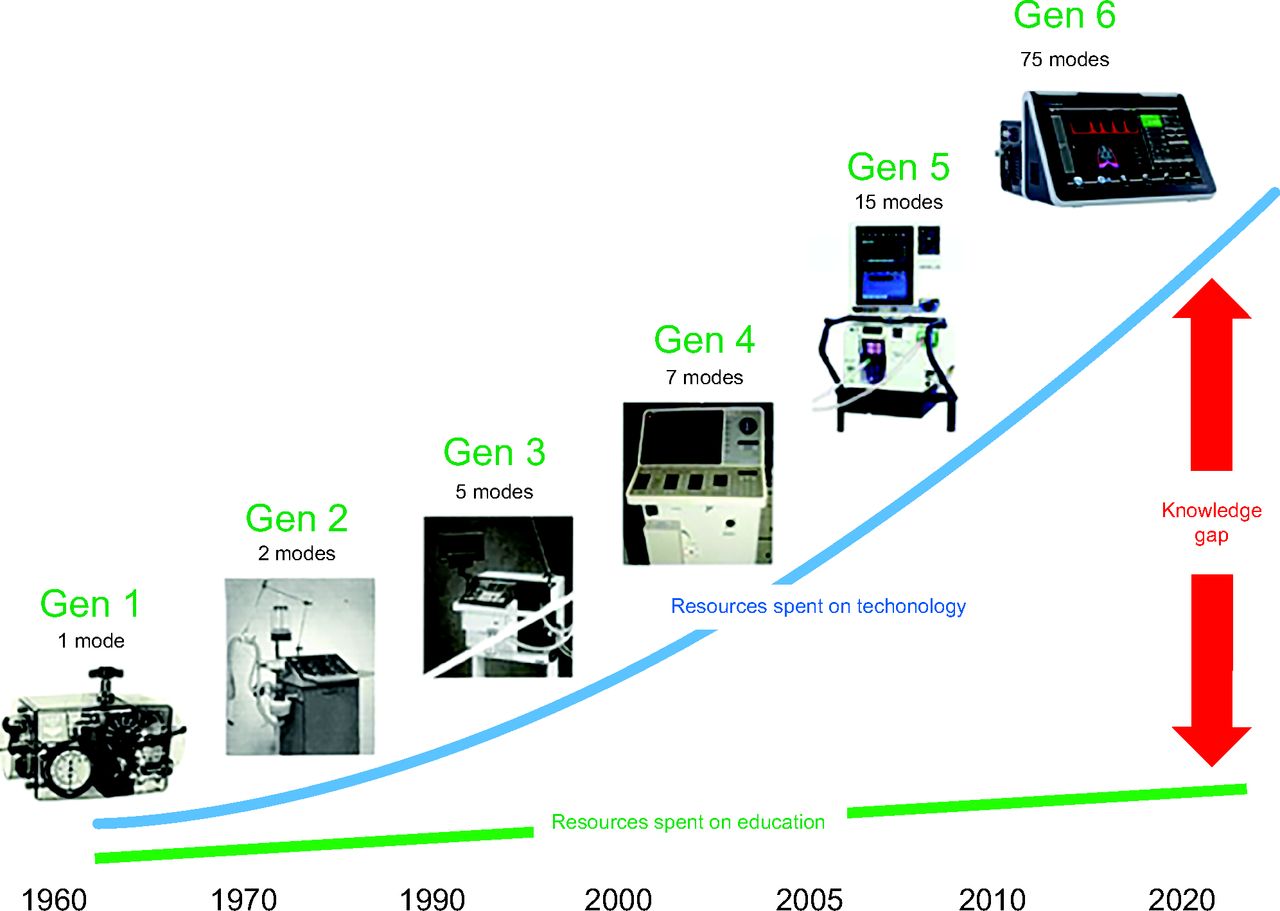
The complexity of ventilator technology has increased dramatically over the last half century (a span of only a single professional lifetime). The first generation of popular mechanical ventilators before the 1970s was mostly noninvasive devices like the iron lung, whose success was driven by the polio pandemic (Table 1).5 However, there were many positive-pressure devices with a bewildering array of designs, mostly based on bellows or pistons. The bible of mechanical ventilation before 1980 was called Automatic Ventilation of the Lungs by Mushin et al.6 It is a fascinating read and was probably the first book to show pressure, volume, and flow waveforms as performance characteristics under conditions of changing lung mechanics. Around the time of the popularization of ICUs in the United States (1970s), a second generation of commercially popular ventilators arose that offered only one or 2 modes of ventilation. This was true both in the adult and pediatric ICUs. As microprocessors became available in the 1980s, digitally controlled ventilators appeared that had a variety of modes in the third generation. Inexpensive digital displays led to fourth-generation ventilators with integrated graphic displays. The fifth generation gave us ventilators with multiple microprocessors and virtual instrument interfaces. Currently, the sixth generation of ventilators provides many dozens of different modes on a single device, with advanced control, monitoring, and graphics capabilities including use of virtual instrument interfaces, artificial intelligence, esophageal pressure manometry, and volumetric capnography.
Evolution of Intensive Care Ventilators
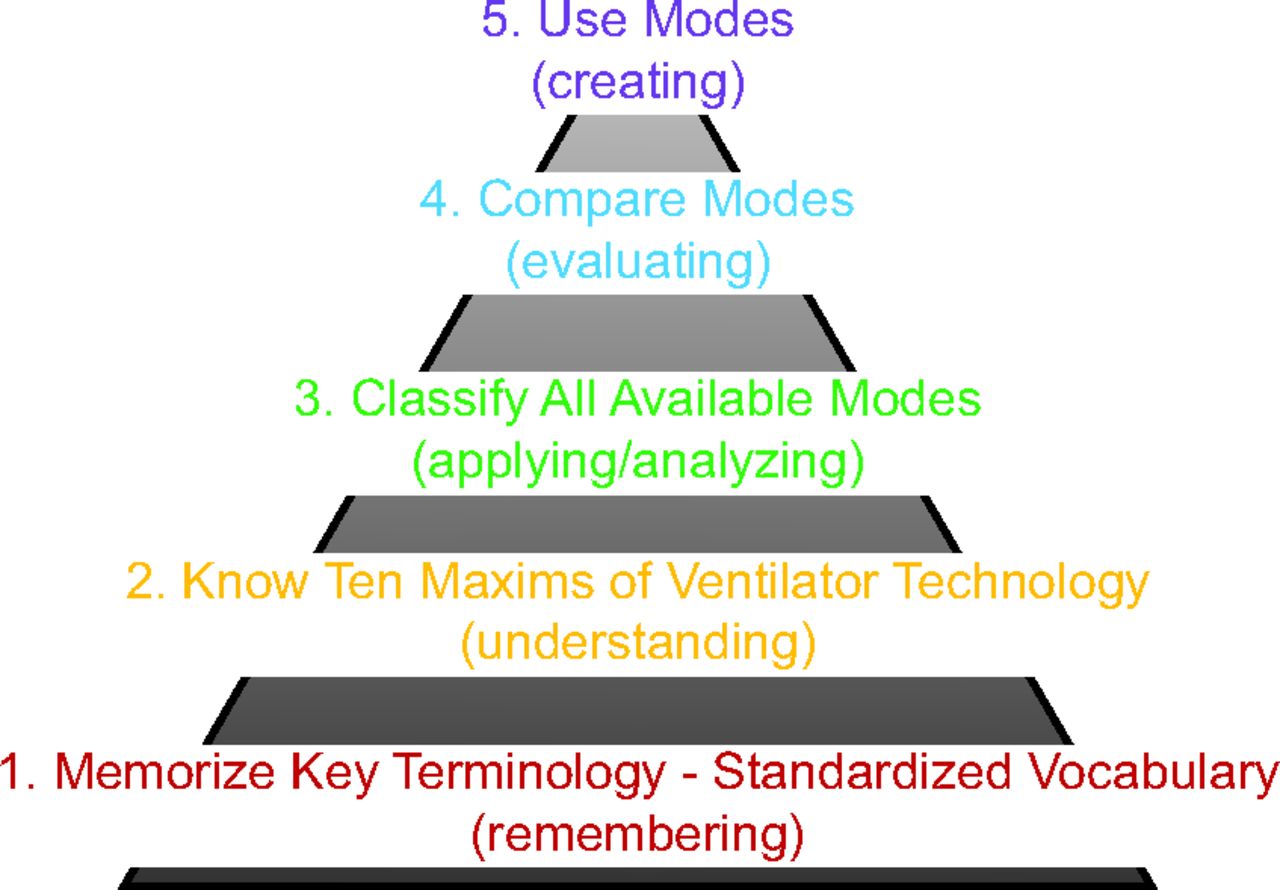
Over the generations of mechanical ventilators, the technological complexity has grown exponentially (Fig. 2). Unfortunately, the educational resources developed to teach mechanical ventilation have not kept pace. As a result, there is a growing knowledge gap on the part of clinicians charged with managing mechanical ventilation. This gap greatly affects patient safety, health care cost, and clinician confidence. Clearly, we have an ever-increasing problem that negatively affects patient care, places an overwhelming burden on our educational systems, and hinders our ability to contribute as health care providers. I am suggesting that we need a new educational paradigm. This new paradigm is represented by a pyramid of skills (Fig. 3) that the clinician needs to know to be an expert in the technology of mechanical ventilation. Its structure correlates with Bloom’s taxonomy7 (a classification system used to define and distinguish different levels of human cognition). Indeed, it justifies the need for a taxonomy for modes of ventilation based on fundamental principles of physics and mathematics. The idea is that you are expected to be able to use all modes. Before that, you must be able to understand, compare, contrast, and recommend all modes. Before that, you must be able to recognize and classify all modes. To do that, you must have the fundamental understanding of 10 basic maxims of mechanical ventilation. And before anything else, you must memorize the definitions of the terms that are used to create the 10 maxims. Note that this pyramid just addresses the technology of mechanical ventilation, not the practice. Think of it as learning how to read sheet music versus play notes on a musical instrument. Using a ventilator, like playing music, is a related but fundamentally different topic.

The growing knowledge gap.

Pyramid of skills to master mechanical ventilation. Words in parentheses correspond to Bloom’s taxonomy.
You may be wondering why the need for this paradigm. Doesn’t it just make things more complicated? Let’s use a simple analogy. Suppose you perform an internet search for headache medicines. Google provides 3 options, without qualification, as if they were equivalent. They all have different brand names, which do nothing to inform you of performance. This is analogous to how a ventilator offers a list of modes. But you know that drugs have generic names. You look on the labels and find that one brand is actually a mixture of 3 different drugs, one has 2, and one is just a pure drug. And furthermore, one label even gives the drug classification as pain reliever in addition to the generic name. Imagine a world where there were no generic names for the thousands of different brand names of drugs. If you were responsible for using drugs for patient care, you would, by necessity, be limited to using a small number of drugs and would find it difficult to add new drugs to your toolbox. Well, that is exactly where we stand with hundreds of brand names for modes of ventilation. Most clinicians (let alone researchers, educators, and manufacturers) are not aware of the mode taxonomy, and so naturally they understand and use only a small number of modes. Compare this to the relatively much larger number of drugs the average clinician knows (and uses) and the problem becomes obvious.
There are many thousands of prescription drug products approved by the United States Food and Drug Administration for marketing. The world of pharmacology has dealt with this challenge in 3 steps. First is to create a taxonomy to classify types of drugs and distinguish among arbitrary brand names. Second is to create a science of pharmacodynamics to describe the physiological effects of different drugs. Third, there is the study of pharmacokinetics to understand how the body interacts with drugs. Whereas 500 mode names may seem insignificant in comparison to thousands of drug names, certainly the need for organization is evident. The first step would be to create a taxonomy or classification system for modes. This helps us to distinguish which ones are the same and which ones are different among all the different brand names. Second, we can create a system of concepts to help us understand the general design principles of ventilators as a basis for the taxonomy. Third, we can create another taxonomy for describing the physics of patient-ventilator interactions (PVIs) in terms of synchrony versus discordance.8 This approach can be the basis of a standardized educational program for mechanical ventilation. And by the way, standardized educational programs are essential for things like basic life support and advanced life support training in medicine. They are standardized because lives depend on the application of consistent, proper technique. We should think no less of mechanical ventilation. Yet physicians and nurses are not taught this subject in universities. And you cannot even find 2 respiratory therapy programs in the same city that teach the subject the same way, despite using the same textbooks.
The SEVA Program
With that introduction, I will now describe the education solution created at our hospital. It is called the SEVA program (pronounced sāy-va, and trademarked by Cleveland Clinic). SEVA stands for standardized education for ventilatory assistance. It is also a Sanskrit word that means selfless service (consistent with our hospital’s slogan of “patients first”). SEVA was conceived and developed by Dr Eduardo Mireles-Cabodevila and myself at Cleveland Clinic. Many other physicians and RTs have contributed over the last decade. The vision of the SEVA program is to provide a unique platform for standardizing training by unifying the concepts of physics, physiology, and technology of mechanical ventilation. The mission is to use both online and in-person simulation-based instruction that has both self-directed and instructor-led components to elevate the skills of health care providers to the mastery level. We believe that standardized education will yield better understanding of current and future ventilation technology. Better understanding will lead to better application of all ventilators and modes as well as related monitoring tools. Better education will lead to better communication among caregivers, better orders and charting in medical records, and more efficient decision-making at the bedside. And of course, the ultimate motivation is better patient care, including shorter duration of ventilation and fewer adverse events.
The roots of the taxonomy for modes of ventilation can be traced back to the early 1990s when I was writing a textbook on respiratory care equipment with my colleagues Richard Branson and Dean Hess.9 That was the first time the equation of motion (EoM) was used as the theoretical basis for classifying modes of ventilation. But the formal birth was with a paper published in Respiratory Care in 2012 entitled Determining the Basis for a Taxonomy of Mechanical Ventilation.10 Believe it or not, it was an adaptation of my master’s thesis. My colleagues and I followed this paper with a complete description of the mode taxonomy based on what we called the 10 fundamental maxims. These maxims are the essential concepts required to understand the design and function of ventilators and the classification of modes. They provide the theoretical framework upon which the taxonomy is built. Of course, being able to identify modes is only one level of skill. Ultimately, we need to be able to assess the patient’s needs and support them with the most appropriate mode. Therefore, we wrote a paper providing a rational framework for selecting modes based on how well their technical features serve the 3 goals of ventilation.11 These goals are safety (adequate gas exchange and lung protection), comfort (maximum patient-ventilator synchrony) and liberation (minimum duration of ventilation with the fewest adverse events). Most recently, we have created another taxonomy for PVIs to unify the clinical and research observations of future studies and educational materials.8 Over the last 10 years, the fundamental concepts of SEVA have been adopted, without modification, by nearly every textbook on mechanical ventilation and general respiratory care (see Supplemental Material, References; see related supplementary materials at http://www.rcjournal.com). This system has also been adopted by ECRI as a means of fair comparison of modes among different ventilator brands.12 ECRI reports are used by hospitals when making purchase decisions. This infrastructure of published works provides educators a practical means of standardizing education across many different teaching venues.
What follows is a brief overview of the SEVA curriculum (Table 2). The first 3 levels of SEVA reside on the learning management system of Cleveland Clinic (called MyLearning). These are free and open to the public. Each has post tests, with a score of 80% required to progress to subsequent courses. The remaining courses are in-person and instructor led in a simulation center.
SEVA Courses
SEVA-basic
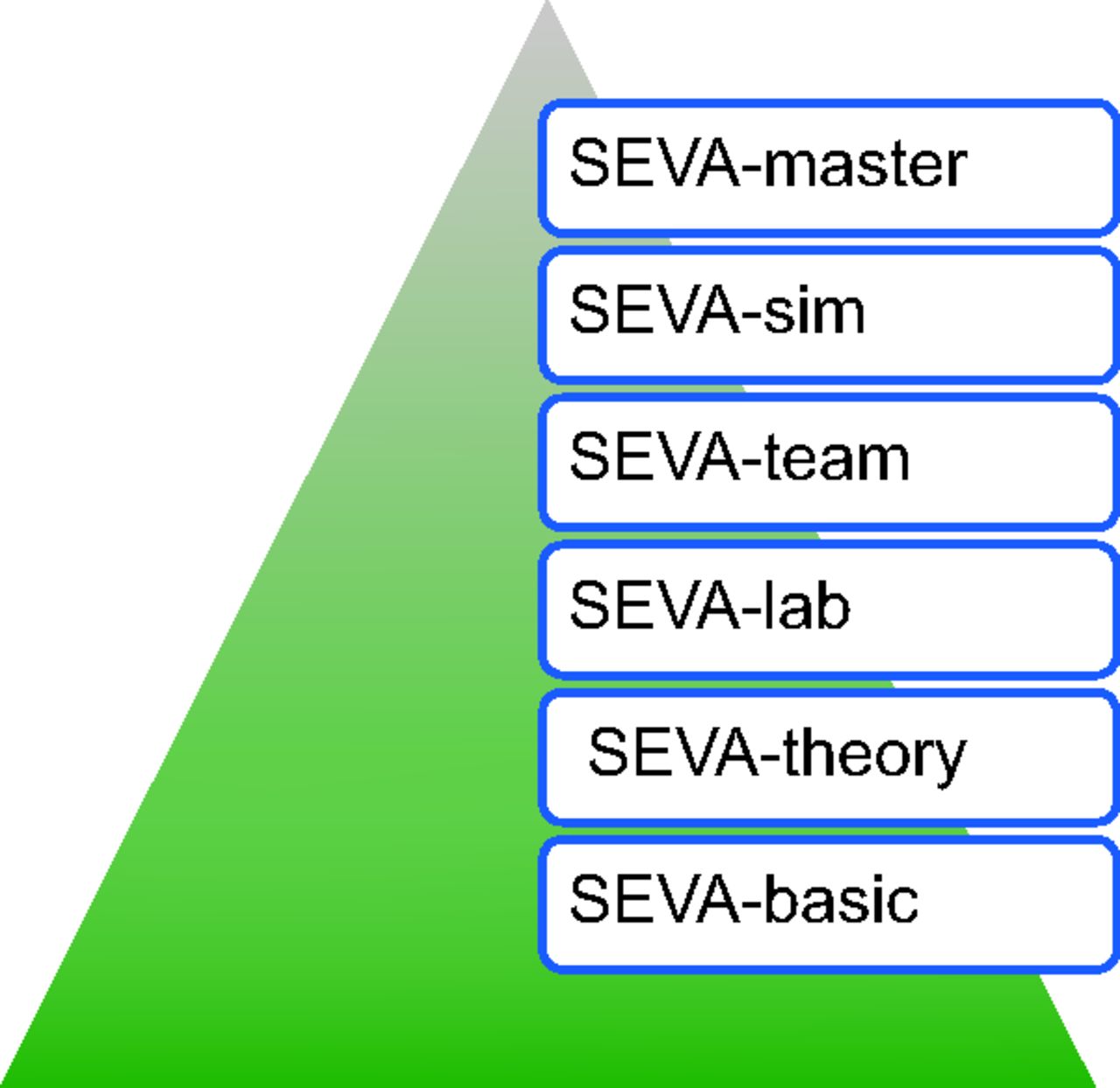
The SEVA program is a progressive system of 6 sequential courses starting from an assumption of no prior knowledge and proceeding to full mastery of advanced techniques (Fig. 4). The first module is called SEVA-basic. It introduces the main concepts from subsequent levels and contains simple versions of material found in SEVA-theory and SEVA-team. The modules of this course are described briefly below. At Cleveland Clinic, the SEVA-basic course is required for all RTs who work in the ICUs. The full SEVA program is required at Cleveland Clinic for physicians in the pulmonary and critical care fellowship.

The SEVA program is a progressive system of 6 sequential courses.
Equation of Motion
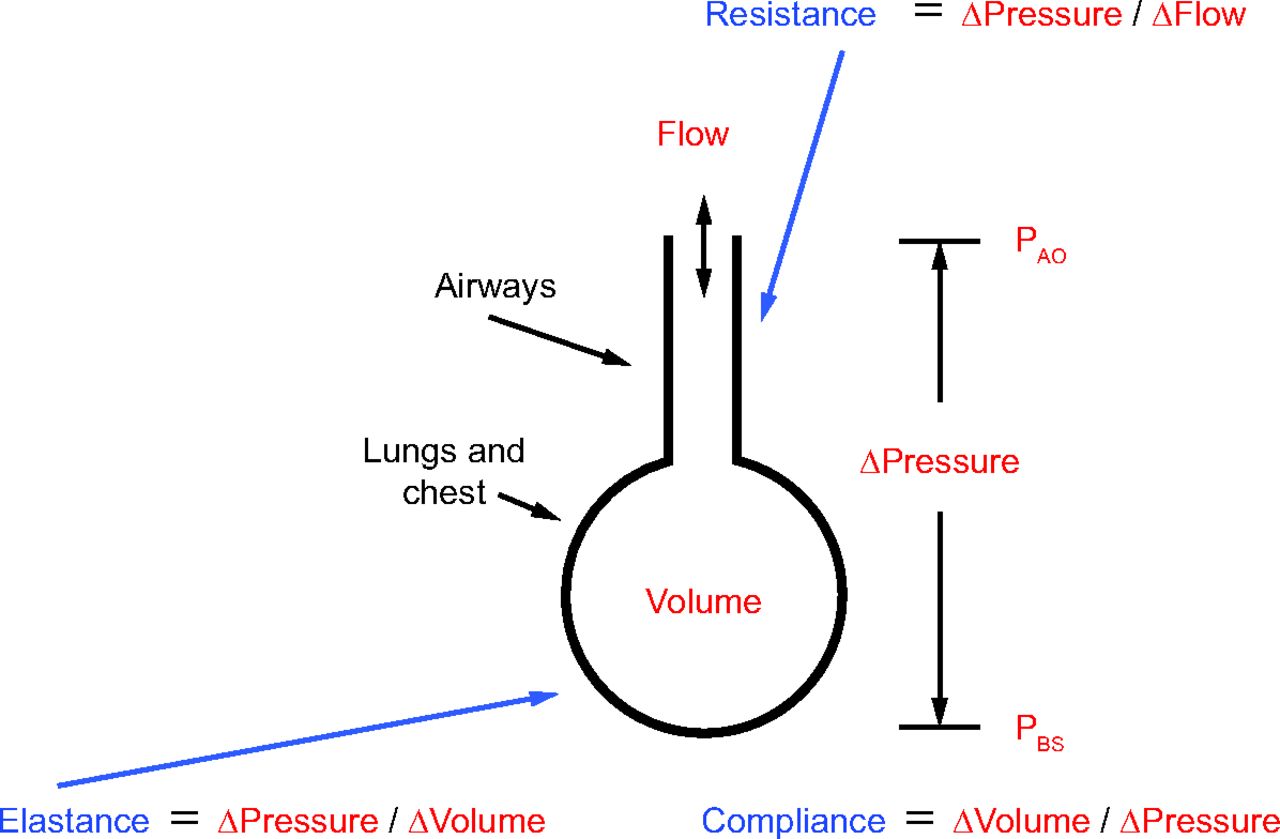
Modes of ventilation and interpretation of PVIs (ie, waveform interpretation) are most easily understood by invoking a simple model of the respiratory system. This model is composed of a single-flow conducting tube representing the airways and a single elastic compartment representing the chest wall and lungs (Fig. 5). The advantage of this model is that it allows for simple representation of the respiratory system in terms of the mechanical properties of resistance and compliance as relations among the variables of pressure difference, volume, and flow. Pressure, volume, and flow as functions of time are related by a mathematical model called the Equation of Motion for the respiratory system. This course introduces the EoM (described in detail below) and how it is used. Additionally, the concept of elastic and resistive loads (derived from the EoM) is introduced as the basis for interpreting ventilator waveforms.

The single compartment model of the lungs. PAO = pressure at the airway opening; PBS = pressure at the body surface.
Taxonomy for Modes of Ventilation
A standardized vocabulary for mechanical ventilation is described and used as the basis for the mode taxonomy (see Supplemental Material, Glossary; see related supplementary materials at http://www.rcjournal.com). The SEVA-theory course derives this taxonomy in great detail (see below). The SEVA-basic course provides an overview of the components of a mode including the control variable, the breath sequence, and the targeting scheme(s). With the skills to identify a mode, the learner is then introduced to the idea of choosing the most appropriate mode based on the primary goal of ventilation at the moment (ie, safety, comfort, or liberation). These ideas are developed more thoroughly in the SEVA-team course (see below).
Waveforms and Measurements
Objectives for this module of SEVA-basic include learning to identify idealized pressure, volume, and flow waveforms for both volume control (VC) (constant and descending ramp flow waveforms) and pressure control (PC) modes. The definition of the time constant is introduced along with how to use it to identify abnormalities in ventilator waveforms. The learner is instructed on the use of inspiratory and expiratory hold maneuvers for the purposes of measuring plateau pressure (Pplat), total PEEP (PEEPtot), and intrinsic or auto-PEEP (PEEPauto). These measurements are then used to calculate resistance, compliance, and tidal pressure13 (also known as driving pressure).
Patient-Ventilator Interactions
In this module of SEVA-basic, the student learns to interpret ventilator graphics by examining pressure, volume, and flow waveforms as described in our paper on the taxonomy of PVIs.8 These skills are developed and practiced in depth in SEVA-teams (see below). At the end of this module, the student is introduced to the 3-step procedure for waveform interpretation that includes (1) determining the mode taxonomic attribute grouping (TAG), (2) identifying the load (elastic, resistive, or muscle pressure [Pmus]), and (3) naming the status of the PVIs for each phase of the breath (ie, trigger, inspiration, cycle, expiration).
SEVA-theory
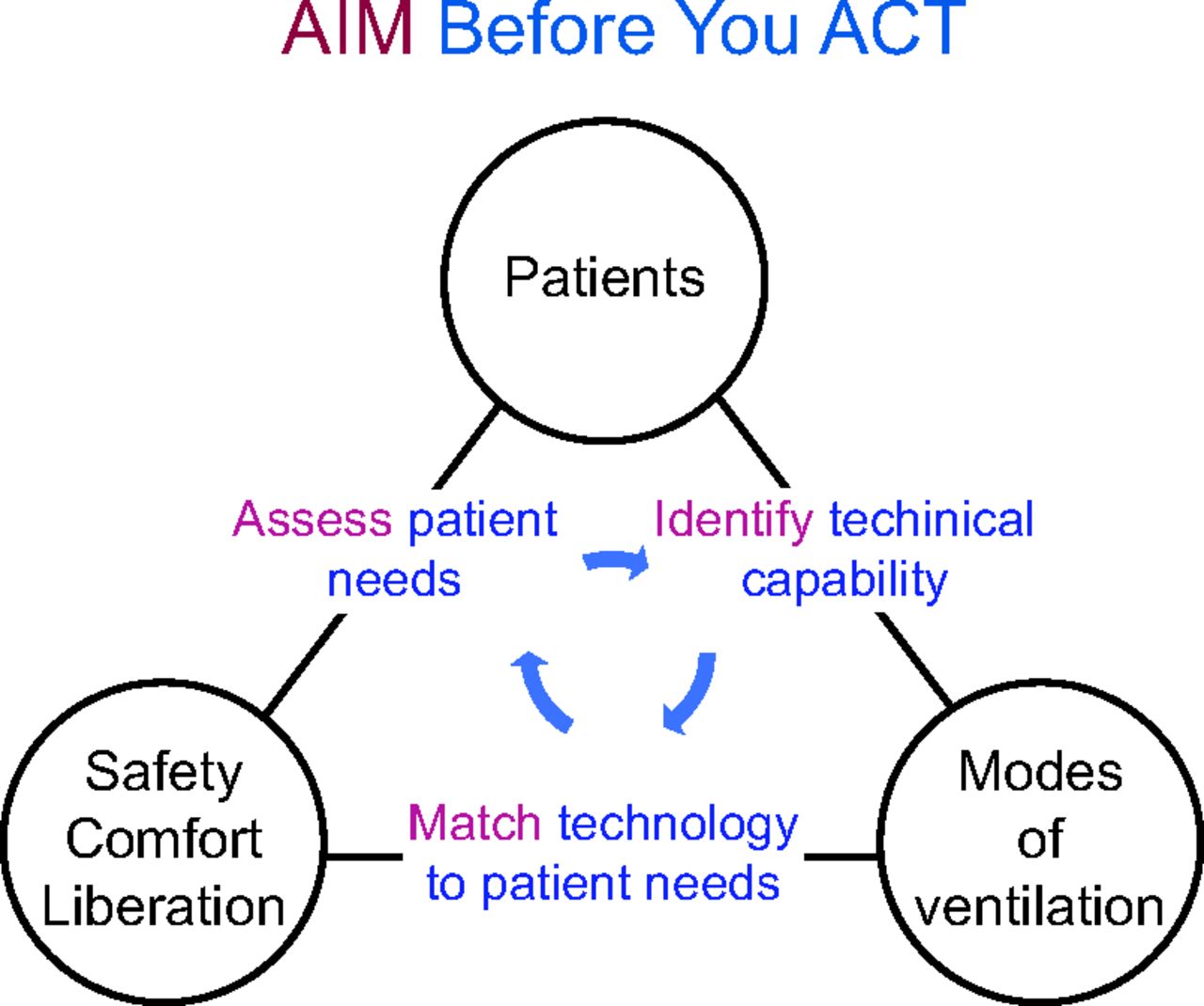
SEVA-theory is the heart of the SEVA program. It begins with a brief explanation of the AIM Before You ACT rubric (Fig. 6). It illustrates the relation between the patient, the primary goal for the patient (safety, comfort, or liberation), and the possible treatments (modes of ventilation). The idea is that you AIM (Assess patient to determine the goal, Identify the technical capabilities of the available modes, and then Match the primary goal) before you ACT (Apply, Considered, Technology). This general rubric applies to everything we do in the form of patient treatment.

AIM Before You ACT rubric. With permission from Cleveland Clinic.
After that, the course is organized in terms of 10 fundamental maxims that form the theoretical framework for the taxonomy of modes.14 Figure 7 shows the dashboard that appears to students in the MyLearning environment. The 10 maxims are described in Table 3. Key teaching points for the maxims are as follows:

SEVA program dashboard at MyLearning, Cleveland Clinic’s learning management system. With permission from Cleveland Clinic.
Ten Basic Maxims for Understanding Ventilator Operation
The Ten Maxims
Maxim 1: The Breath.
The breath is defined by the ventilator in terms of the flow-time waveform (Fig. 8). The horizontal axis is time, so various periods can be defined that are important ventilator settings. By convention, flow in the positive direction is inspiration and flow in the negative direction is expiration.

The breath is defined by the flow-time waveform. With permission from Cleveland Clinic.
Maxim 2: The Assisted Breath.
Work per breath during mechanical ventilation is defined graphically as the area between the pressure-volume curve and the volume axis (Fig. 9). A breath (ie, the patient) is “assisted” if the ventilator does some portion of the work of breathing (WOB). This is observed as airway pressure rising above baseline (PEEP) during the inspiratory time (TI). A breath is “loaded” if the patient does some work on the ventilator system. This is observed as airway pressure falling below baseline during inspiration. A common misconception is that an assisted breath is any patient-triggered breath, which is obviously not true for demand-valve CPAP systems. Some people incorrectly use the word assisted to imply that the patient assists the ventilator by simply triggering the breath. Most assuredly the ventilator assists the patient, not the other way around.

The assisted breath is defined in term of work. Work is defined graphically as the shaded area between the pressure-volume curve and the volume axis.
Maxim 3: Assistance by Volume or Pressure Control.
The theoretical framework for understanding virtually all physical interactions between the ventilator and the patient is a mathematical model called the EoM for the respiratory system:
 (1)
(1)
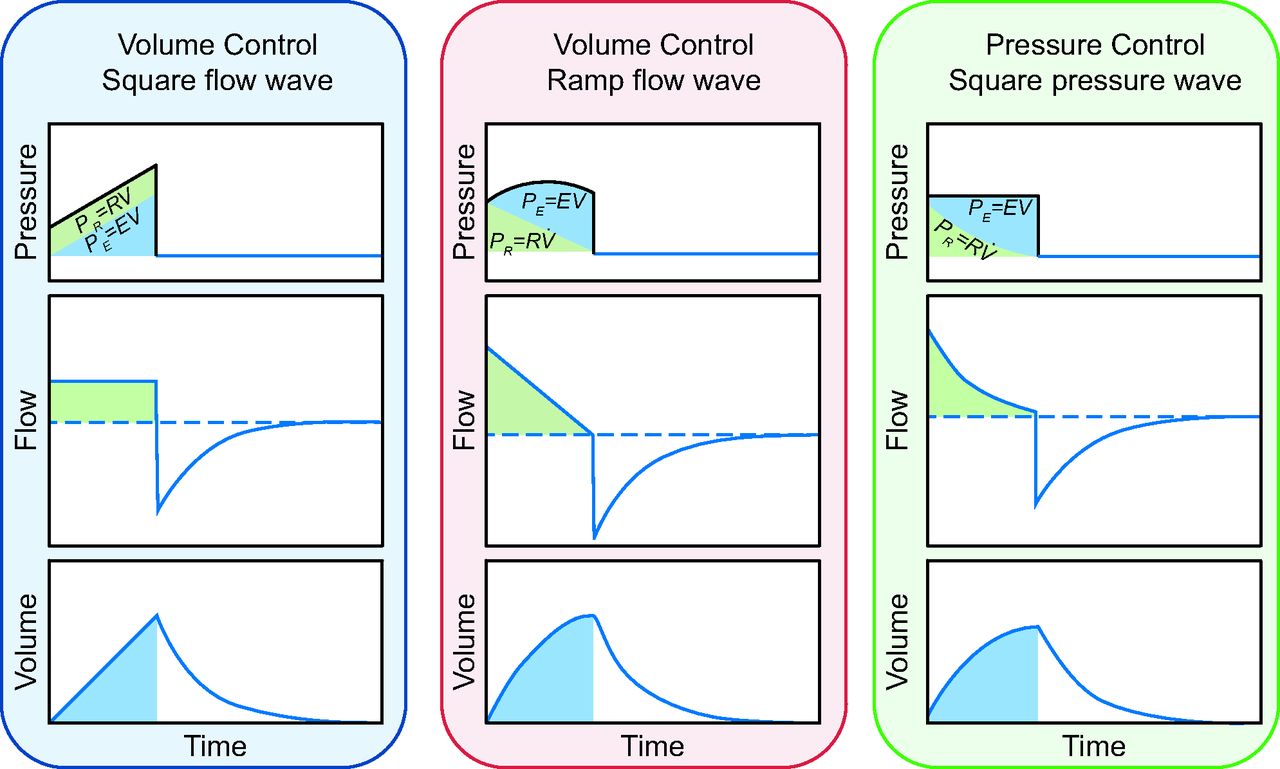
This equation relates pressure, P, volume, V, and flow, V̇, as variables expressed as continuous functions of time, t, whereas elastance (E = ΔP/ΔV) and resistance (R = ΔP/ΔV̇) are parameters of the equation that have constant values. Often compliance, C, is used instead of E (C = ΔV/ΔP). In this form, P is airway pressure relative to PEEP; V is lung volume relative to end-expiratory lung volume (ie, functional residual capacity plus the volume due to PEEP), and V̇ is flow relative to zero. This simplified form of the equation assumes that expiration is complete (no PEEPauto). Pvent is the pressure generated by the ventilator to deliver flow and volume. Pmus is the pressure generated by the patient’s ventilatory muscles. If Pvent = 0 and Pmus > 0, the equation represents unassisted breathing. If Pmus = 0 and Pvent > 0, the equation represents full ventilatory support. If both variables are > 0, then both the ventilator and the patient contribute to the WOB. The term E × V is called the elastic load, and the term R×V̇ is called the resistive load. These terms will be important later in learning how to interpret ventilator waveforms.
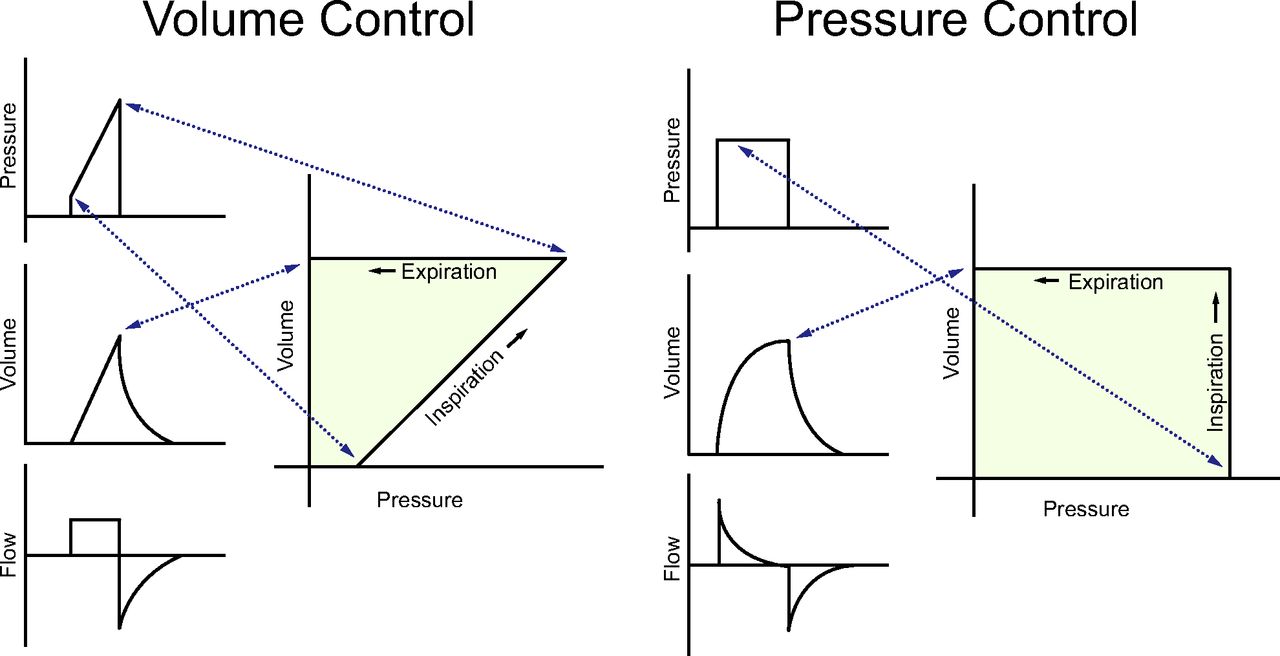
The EoM is implied in the design of every ventilator. Indeed, ventilator waveforms are simply graphs of the equation (Fig. 10). SEVA-theory relies heavily on use of this model. The EoM is a differential equation (specifically, a first-order, linear differential equation with constant coefficients), requiring skills in calculus to fully appreciate. However, the course provides an intuitive understanding of the mathematics with practical applications. Nothing more than high school algebra is required to pass the course.

Ventilator waveforms for volume control and pressure control are graphs of the equation of motion. Green areas under the pressure waveform represent the resistive load, and the blue areas represent the elastic load. With permission from Cleveland Clinic.
The EoM provides the rationale for dividing all modes into 2 broad classes, VC and PC. VC means that both volume and flow are preset. Setting tidal volume (VT) is a necessary but not sufficient criterion for classifying a mode as a form of VC because some modes of PC allow the operator to set a target VT but allow the ventilator to determine the flow (see adaptive targeting schemes below). Similarly, setting flow is also a necessary but not sufficient criterion; some PC modes allow the operator to set the maximum inspiratory flow, but the VT depends on the inspiratory pressure target and respiratory system mechanics.
PC means that inspiratory pressure as a function of time is preset. In practice, this currently means presetting a particular pressure waveform, eg, Pvent (t) = constant, or inspiratory pressure is set to be proportional to patient inspiratory effort measured by various means. For example, Pvent (t) = NAVA level × EAdi (t) where NAVA stands for neurally-adjusted ventilatory assist and EAdi stands for electrical activity of the diaphragm (see Servo targeting scheme below). In a passive patient, after setting the form of the pressure function (ie, the pressure waveform), volume and flow depend on E and R.
Equation 1 can be solved to show various pressures, volumes, and flows as functions of time during inhalation and exhalation. For example, the expression for flow during passive exhalation is
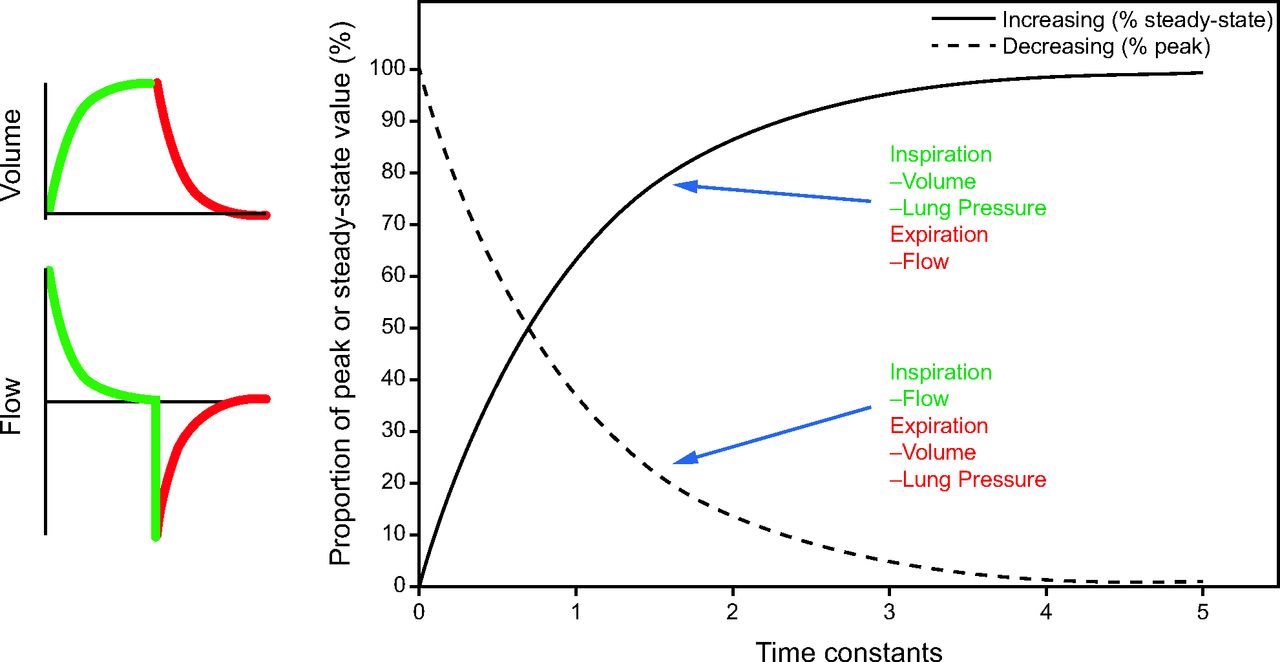
 (2)where Pplat = plateau pressure during an inspiratory hold maneuver; PEEPset = PEEP set on the ventilator; e is the base of the natural logarithms (e ≈ 2.72), and t is the time from the start of expiration. The expression Pplat − PEEPset divided by R is peak expiratory flow.13 The product of resistance and compliance, RC, has the units of time (s). When t = RC, the expression e-t/RC equals approximately 0.37. This means that when expiratory time (TE) equals RC, peak expiratory flow has dropped by 63%. It can be shown that in another unit of time equal to RC the flow drops by another 63% and so on. Hence the term RC, called the time constant, is a useful way of describing the rate of change in exponential functions of time (Fig. 11). In this example, a short time constant means that expiration happens quickly (with less chance of gas trapping) and vice versa. This concept becomes very important later when learning to interpret ventilator waveforms.
(2)where Pplat = plateau pressure during an inspiratory hold maneuver; PEEPset = PEEP set on the ventilator; e is the base of the natural logarithms (e ≈ 2.72), and t is the time from the start of expiration. The expression Pplat − PEEPset divided by R is peak expiratory flow.13 The product of resistance and compliance, RC, has the units of time (s). When t = RC, the expression e-t/RC equals approximately 0.37. This means that when expiratory time (TE) equals RC, peak expiratory flow has dropped by 63%. It can be shown that in another unit of time equal to RC the flow drops by another 63% and so on. Hence the term RC, called the time constant, is a useful way of describing the rate of change in exponential functions of time (Fig. 11). In this example, a short time constant means that expiration happens quickly (with less chance of gas trapping) and vice versa. This concept becomes very important later when learning to interpret ventilator waveforms.

Graph showing how the time constant describes the change of exponential waveforms during mechanical ventilation. With permission from Cleveland Clinic.
Maxim 4: Trigger and Cycle Events.
The start of inspiration (start of positive flow) is called the trigger event. The end of inspiration (start of negative flow or expiration flow) is called the cycle event. The ventilator monitors a variable, like time, pressure, or flow, and starts or stops inspiration when the variable reaches a preset threshold. The threshold value is determined by the sensitivity setting. Note that a high threshold value corresponds with a low sensitivity setting and vice versa.
Maxim 5: Machine Versus Patient-Initiated Trigger and Cycle Events.
Patient triggering means starting inspiration based on a patient trigger signal independent of a ventilator-generated trigger signal.
Patient cycling means ending (TI) based on signals representing the patient determined components of the EoM, (ie, elastance or resistance, and including effects due to inspiratory effort). Flow cycling is a form of patient cycling because the rate of flow decay to the cycle threshold, and hence the TI, is determined by patient mechanics (ie, the time constant and effort).
Note that it is possible for a passive patient to both trigger and cycle inspiration based only on the resistance and compliance of the respiratory system.15
Ventilator triggering means starting inspiratory flow based on a trigger signal (usually time) from the ventilator, independent of a patient trigger signal.
Ventilator cycling means ending TI independent of signals representing the patient determined components of the EoM.
Maxim 6: Mandatory and Spontaneous Breaths.
A spontaneous breath is a breath for which the patient retains substantial control over timing. This means that the start and end of inspiration are determined by the patient, independent of any ventilator settings for TI and TE. That is, the patient both triggers and cycles inspiration. A spontaneous breath may occur during a mandatory breath (eg, Airway Pressure Release Ventilation). A spontaneous breath may be assisted or unassisted. Indeed, the definition of a spontaneous breath applies to normal breathing as well as mechanical ventilation. Some authors use the term spontaneous breath to refer only to unassisted breaths, but that is an unnecessary limitation that prevents the word from being used as a key term in the mode taxonomy.
A mandatory breath is a breath for which the patient has lost some control over timing (ie, frequency or TI). This means a breath for which the start or end of inspiration (or both) is determined by the ventilator, independent of the patient. In other words, the ventilator triggers and/or cycles the breath. A mandatory breath can occur during a spontaneous breath (eg, high-frequency jet ventilation). A mandatory breath is, by definition, assisted (ie, the patient is assisted by the ventilator, not the other way around).
Maxim 7: Breath Sequences.
A breath sequence is a particular pattern of spontaneous and/or mandatory breaths. The 3 possible breath sequences are continuous mandatory ventilation (CMV), intermittent mandatory ventilation (IMV), and continuous spontaneous ventilation (CSV). CMV, commonly known as “Assist/Control,” is a breath sequence for which spontaneous breaths are not possible between mandatory breaths because every patient trigger signal produces a ventilator cycled inspiration (ie, a mandatory breath). IMV is a breath sequence for which spontaneous breaths are possible between mandatory breaths. Ventilator-triggered mandatory breaths are delivered at a preset frequency. The mandatory breath frequency for CMV may be higher than the set frequency but never below it (ie, the set frequency is a minimum value). In some PC modes on ventilators with an active exhalation valve, spontaneous breaths may occur during mandatory breaths.
Therefore, the defining characteristic of CMV is that spontaneous breaths are not permitted between mandatory breaths. In contrast to CMV, the set frequency of mandatory breaths for IMV is the maximum value because in some forms of IMV spontaneous breaths suppress mandatory breaths (see the different types of IMV described below).
CMV and CSV are made possible by use of a trigger window. This is a period of time equal to the TE (minus a short refractory period to prevent inadvertent double triggering) during which a patient trigger signal will start a mandatory breath (in CMV) or a spontaneous breath (CSV or IMV). IMV is made possible by use of a synchronization window. A synchronization window is a short period (eg, 5 ms) at the end of a preset TE (ie, as a function of preset TI and breath rate) during which a patient signal may be used to synchronize the trigger event with a patient inspiratory effort signal. Generally, such an inspiration is machine cycled and hence results in a patient-triggered mandatory breath. When this happens in IMV, it is called synchronized IMV, SIMV. Trigger and synchronization windows have been described in more detail elsewhere.16
There are 4 different types of IMV.16 Without an understanding of these types, it is not possible to appreciate the evolution of modes from simple, manually adjusted types to increasingly more automatic varieties, making possible more advanced modes.
IMV(1): Mandatory breaths are always delivered at the set frequency (eg, SIMV VC mode on Medtronic PB 840 ventilator).
IMV(2): Mandatory breaths are suppressed when the spontaneous breath frequency is > than the set frequency (eg, BiPAP S/T mode on Philips Respironics V60 ventilator).
IMV(3): Mandatory breaths are suppressed when the measured minute ventilation (ie, product of breath frequency and VT) is > a preset threshold due to spontaneous breaths (examples include Mandatory Minute Volume mode and Adaptive Support Ventilation [ASV] mode).
IMV(4): Individual mandatory breaths may be suppressed due to the effects of the patient’s inspiratory efforts on trigger and cycle events. This currently may happen in 2 ways. In both cases, a scheduled mandatory breath (ie, one that is machine triggered by a set rate) becomes patient triggered so that the first criterion of a spontaneous breath is satisfied. In the first case, a VC inspiration switches to PC due to high inspiratory effort (see dual targeting below) and becomes flow (patient) cycled, and hence this breath becomes spontaneous (ie, both triggered and cycled by the patient). This happens for VC modes on Servo ventilators (Getinge, Göteborg, Sweden). In the second case, the mandatory inspiration was already set to be patient cycled (by flow), and hence again the mandatory breath becomes a spontaneous breath. This happens for a mode called Pressure A/C with Flow Cycle on the Avea ventilator (Vyaire Medical, Mettawa, Illinois).
Maxim 8: Ventilatory Patterns.
Maxim 8 is simple but fundamental. It says that combining the control variable with the breath sequence yields 5 basic ventilatory patterns found on all ventilators. These are VC-CMV and VC-IMV, plus PC-CMV, PC-IMV, and PC-CSV. VC-CMV is not possible because VC implies machine cycling, so there can never be a VC spontaneous breath.
Maxim 9: Targeting Schemes.
A target is a predetermined goal of ventilator output, such as parameters of the pressure, volume, and flow waveforms (eg, peak inspiratory pressure/PEEP, VT, and peak inspiratory flow, respectively).14 A targeting scheme is a model of the relationship between operator inputs and ventilator outputs to achieve a specific ventilatory pattern, usually in the form of a feedback control system.17,18 Examples of targets and targeting schemes are shown in Table 4. A full description of the various targeting schemes is beyond the scope of this paper but has been described extensively elsewhere.4,14
Example Targeting Schemes and Targets
Maxim 10: Mode Taxonomy.
We must distinguish mode names (ie, brand names invented by manufacturers for marketing purposes) from mode classifications for the same reasons we must distinguish drug brand names from generic names. Failure to do this introduces many problems, including inaccuracy in research comparing modes.
Maxim 10 brings together the concepts from the other maxims to create a formal taxonomy for modes of ventilation.14 There are 3 simple steps for classifying any mode: (1) identify the control variable, (2) determine the breath sequence, and (3) specify the primary and secondary targeting schemes for mandatory and spontaneous breaths, respectively. Thus, the symbol for a mode classification (ie, the TAG) has 3 components representing (1) the control variable (VC or PC for mandatory breaths), (2) the breath sequence (CMV, IMV, or CSV), and (3) the targeting scheme (s, d, r, a, b, o, i) for both mandatory and spontaneous breaths (if allowed). Specifically, for IMV, at least 2 symbols are used where the first refers to the mandatory breaths and the second to the spontaneous breaths. Figure 12 shows the classification steps for 3 common modes.

Examples of how to classify 3 common modes of ventilation. CMV = continuous mandatory ventilation; SIMV = synchronized intermittent mandatory ventilation; IMV = intermittent mandatory ventilation; CSV = continuous spontaneous ventilation.
All modes on all ventilators used in the United States have been classified using the mode taxonomy in a recent textbook.4 The database used to write this book is available on a telephone app called Ventilator Mode Map (free download for iPhone and Android).
SEVA-lab
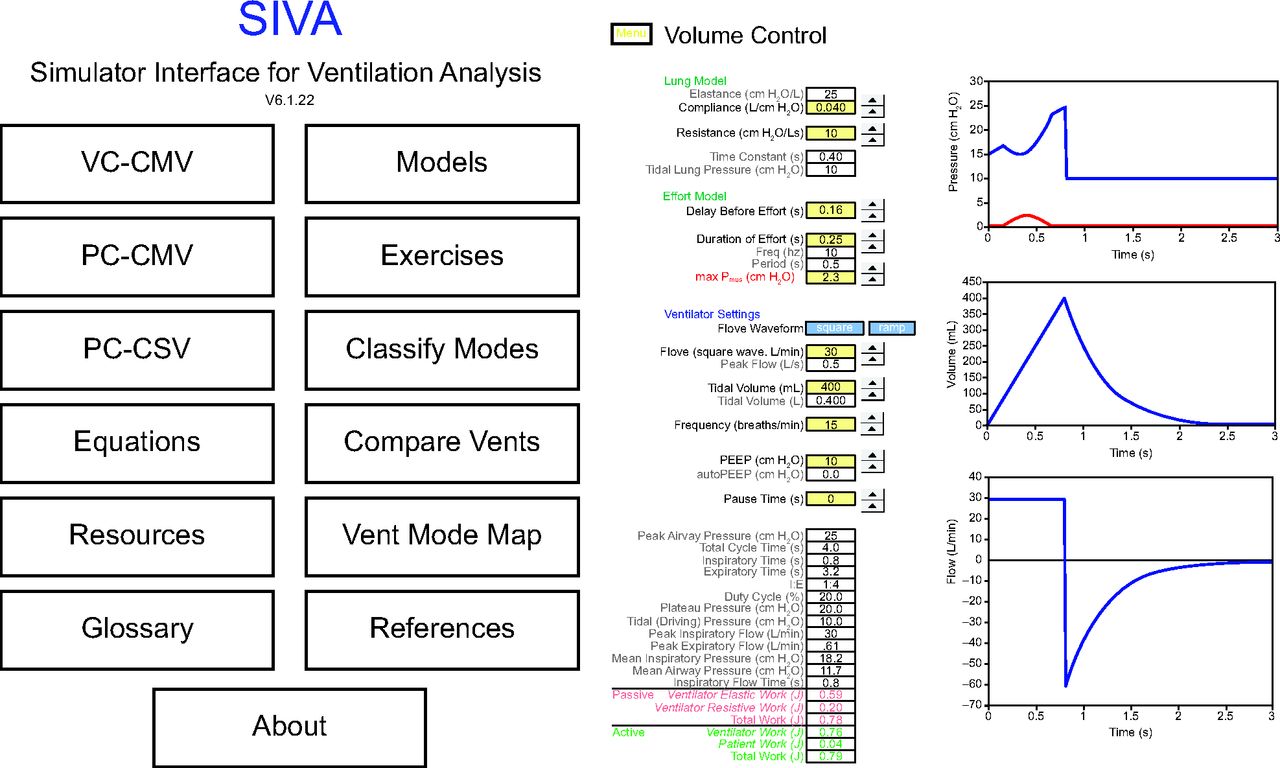
SEVA-lab is a simulated ventilator laboratory experience. It is based on a software patient-ventilator simulator that runs in Microsoft Excel on any computer (Fig. 13). The simulator allows the user to set lung mechanics parameters (resistance, compliance, and Pmus) and adjust ventilator settings for VC and PC modes. The results are displayed on pressure, volume, and flow waveforms as seen on a real ventilator (except that Pmus is also displayed, a variable never shown on ventilators). Learners use a laboratory-style notebook to record the effects of changes in lung mechanics or ventilator settings on ventilator waveforms. Experiments are designed to illustrate all 10 maxims. Each maxim has from 3–10 experiments called events. For each event, the learner first predicts the effects on waveforms of changes in ventilator settings or lung model parameters. These predictions are based on the concepts learned in the SEVA-theory maxims. Then the learner makes the changes on the simulator and records the effects on the pressure, volume, and flow waveforms. After that, the workbook provides the answers and a thorough analysis of the reasons for them. The prediction-answer format allows immediate formative feedback to the learner.

Patient-ventilator simulator. Note the red curve on the pressure graph showing how muscle pressure distorts the pressure generated by ventilator waveform. With permission from Cleveland Clinic.
Each event has the same format: objectives, ventilator settings, lung model parameters, experimental events, analysis. For example, the first event in the workbook is called Maxim 1 – Defining the Breath. It is laid out as follows:
Objectives
Demonstrate the effect of ventilator changes on important time intervals of the breath during VC ventilation.
Ventilator
Mode: VC-CMV
Flow
Square waveform
Flow (L/min) = 30
VT (mL) = 400
Frequency (breaths/min) = 15
PEEP (cm H2O) = 10
Inspiratory pause (s) = 0.2
Patient (ARDS: passive)
Lung model
C (L/cm H2O) = 0.040
R (cm H2O/L/s) = 10
Effort model
Delay before effort (s) = 0
Duration of effort (s) = 0.30
max Pmus (cm H2O) = 0
Event 1–1
Record the following baseline data:
(1) TI
(2) Inspiratory flow time (TIF)
(3) TE
(4) Total cycle time (TCT)
(5) I:E
Analysis.
This event gives practice in recognizing the important time intervals within a breath.
Event 1–2
Objective.
Predict effect of eliminating inspiratory pause time (Tpause) on the following variables (ie, increase, decrease, or no change):
(1) TI (↑ or ↓ or =)
(2) TIF (↑ or ↓ or =)
(3) TE (↑ or ↓ or =)
(4) TCT (↑ or ↓ or =)
(5) I:E (↑ or ↓ or =)
Ventilator
Tpause = 0 s
Data collection
TI
TIF
TE
TCT
I:E
Analysis
Eliminating the Tpause shortens TI
TI = TIF + Tpause
There is no effect on TIF
TIF = TI − Tpause
(Note that TIF always ends when Tpause begins [if there is a pause]).
The TE increases by the amount that TI decreases
(a) TE = TCT − TI
There is no effect on TCT because this is determined by the frequency setting
TCT = 60/f
The I:E gets smaller because TI decreases
I:E = TI/TE
Note that 1:4 < 1:3 because ¼ = 0.25, whereas 1/3 = 0.33
SEVA-team
There are 4 short videos that are required viewing prior to the class. SEVA-team is a unique team-based learning experience. Learners are grouped at tables of 3–5 people with different disciplines (eg, physician, RT, nurse, physician assistant). Participants are given workbooks that briefly review the course content and provide space to write in the answers to questions posed by the instructors. They are given a challenge question and then asked to first write down their own answer, next write down the answer arrived at by consensus for their team, and third record the answer given by the instructors. This format enhances engagement, improves communication skills, and provides insight into how other disciplines think about mechanical ventilation. It is also scalable, both in-person and online (we have trained over 100 people at one time, in-person, at an AARC Congress).
Theory Review
The first module of SEVA-team reviews the material in SEVA-theory and then shows the application to patient assessment and mode selection. The specific focus is on the EoM and the taxonomy for modes of ventilation, including abbreviated mode classifications using TAGs.
Goals of Ventilation and Selecting Modes
SEVA-team also provides the concepts for applying theory in clinical practice. This course introduces the idea that there are only 3 goals of mechanical ventilation, safety, comfort, and liberation (Fig. 14). Once the primary goal has been identified, the appropriate mode is selected based on its technological capabilities to serve that goal.11 Note that a mode like PC-IMV(2)a,a (for example, Automode PRVC to VS) or PC-IMV(3)oi,oi, (example: ASV) could serve as modes for the entire duration of ventilation because they serve all 3 goals at once. Indeed, NAVA as implemented on the Getinge Servo ventilators switches between PC spontaneous breaths with servo targeting and PC mandatory breaths with set-point targeting, depending on the availability of the EAdi signal. As such, it too would be a mode to serve all 3 goals.

The 3 goals of mechanical ventilation change throughout the course of treatment. Only one goal predominates at any time, and that goal determines the most appropriate mode of ventilation. The idea is that each goal has an appropriate mode of ventilation. This is just one example of how modes could be matched to the goals. There are other possibilities and probably better ones depending on availability. With permission from Cleveland Clinic. CMV = continuous mandatory ventilation; IMV = intermittent mandatory ventilation; CSV = continuous spontaneous ventilation.
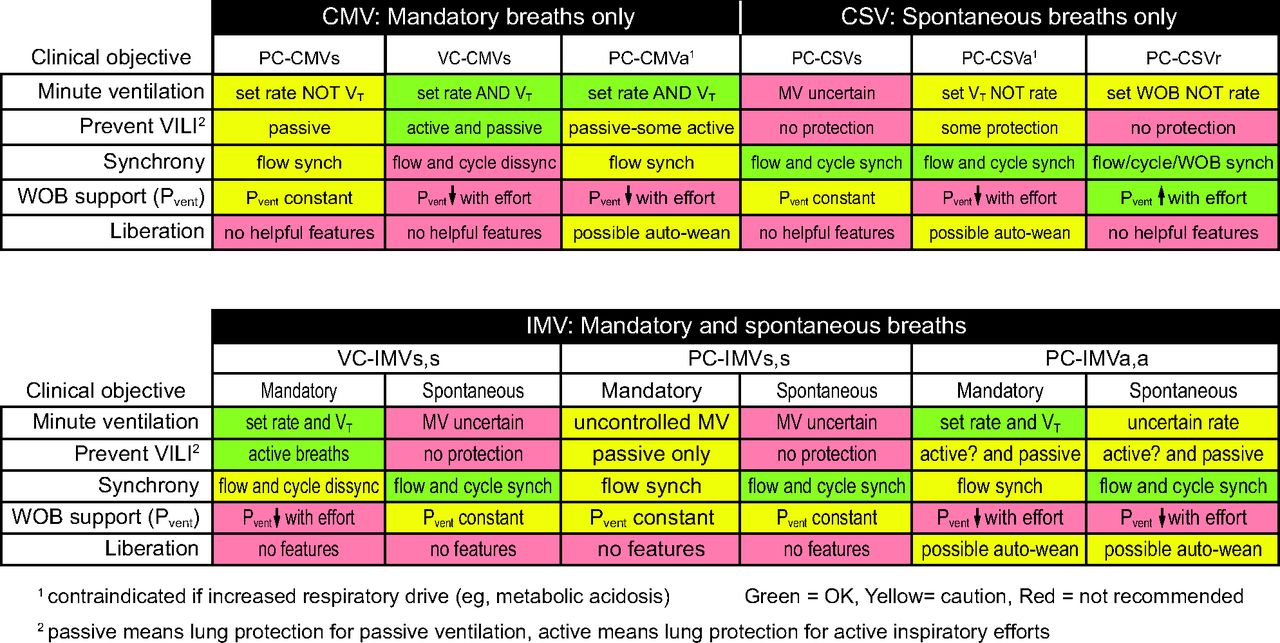
Learners are provided with pocket cards showing a simplified mode selection rubric (Fig. 15). The card instructs them to first select the primary goal for the patient and note the objectives of the goal: safety (provide adequate minute ventilation and minimize risk of lung injury), comfort (maximize patient-ventilator synchrony and assure appropriate work distribution between ventilator and patient), and liberation (minimize duration of ventilation and risk of adverse events). The clinical objectives suggest the most appropriate mode (listed as a generic TAG rather than a name). For example, if safety is the primary goal, then the objectives are to assure adequate gas exchange (ie, minute alveolar ventilation) and minimize risk of ventilator-induced lung injury. Figure 15 shows the example appropriate modes are VC-CMVs and PC-IMVa,a because they assure a safe VT dosage for both active and passive breaths as well as mandatory and spontaneous breaths in the face of changing lung mechanics. On the contrary, the least appropriate example modes are PC-IMVs,s and PC-CSVs because the minute ventilation and VT dosage are uncertain for active and passive breaths as well as mandatory and spontaneous breaths. On the other hand, if comfort is the most important goal, then the objectives are to maximize patient-ventilator synchrony and WOB balance. Therefore, the most appropriate example mode according to the table in Figure 15 is PC-CSVr (eg, proportional assist ventilation or NAVA), although IMV modes could be considered. Note that the table is simplified to include IMV(1) modes only. Otherwise, IMV(2) and IMV(3) modes would be a more robust choice for serving all 3 goals at once.

Mode selection guide. With permission from Cleveland Clinic. PC = pressure control; VC = volume control; CMV = continuous mandatory ventilation; IMV = intermittent mandatory ventilation; CSV = continuous spontaneous ventilation; s = set-point targeting; a = adaptive targeting; r = servo targeting; VT = tidal volume; WOB = work of breathing; Pvent = pressure generated by ventilator during inspiration; VILI = ventilator induced lung injury.
Ventilator Waveform Interpretation
This module applies what the student learned in the previous courses to advanced ventilator graphics interpretation and PVI analysis to assess synchrony problems.
SEVA-sim
There are 3 short videos introducing the clinical module that are required viewing prior to the class. SEVA-sim takes place at a simulation center and uses standard manikins as well as state-of-the-art breathing simulators and real ventilators. In the process, learners become familiar with ventilator “knobology” (ie, how ventilator settings are adjusted with real or virtual knobs and buttons). Learners in teams of 2–6 rotate between 3 stations. The course provides 3 clinical modules (with several progressive scenarios for each) to teach the skills of ventilating patients awakening from anesthesia, with severe obstructive disease and severe restrictive disease. Each module takes about 60 min. Instructors use flow charts to guide the learning experience and standardize the presentation of clinical decision making challenges. Learners are asked to decide upon the most appropriate goal for the patient, select the most appropriate mode, and then consider simulated physiologic responses (eg, blood gases, capnograms, blood pressures, and chest radiographs) to guide mode setting adjustments. Debriefing occurs after each scenario of each module. Learners are encouraged to use the mode selection pocket card (Fig. 15).
Awakening From Anesthesia
The simulated patient is initially paralyzed. Then there will be a gradual increase of inspiratory effort leading to PVI problems (double triggering, work shifting, or large VT). There are 3 scenarios in this module. For scenario 1, the patient is passive; and the learners must identify the goal of ventilation as safety, select an appropriate mode, and adjust settings. For scenario 2, the patient is breathing normally, and the learners must identify the goal as comfort and select the appropriate mode and settings. Finally, in scenario 3, the patient is making vigorous inspiratory efforts; and the learners may select any of the 3 goals of ventilation but with justification and appropriate mode and settings.
Debrief items for this module include selecting appropriate VT dosage, modes that serve the 3 goals, and the impossibility of any mode to cope with extremely high respiratory drive and inspiratory efforts.
Severe Obstructive Disease
The simulated patient is paralyzed throughout the module. The lung simulator is designed to allow separate setting of inspiratory and expiratory resistance to demonstrate generation of PEEPauto with clinically relevant ventilator settings. For scenario 1, the learners must determine the goal and select appropriate mode and settings. The learners should suggest a bronchodilator (or be prompted to do so). The simulator is adjusted to a lower expiratory resistance, and the learner should recognize a change in the expiratory flow waveform. For scenario 2, the learners must recognize the signs of PEEPauto (expiratory flow waveform and shark-fin shape of capnogram) and use an expiratory hold maneuver to measure it. They must then adjust ventilator settings to minimize PEEPauto while maintaining a minute ventilation above 6 L/min. Scenario 3 addresses the idea of how set PEEP can reduce PEEPauto if the applied pressure reduces airway resistance (and hence reduces the respiratory system time constant). Learners perform a PEEP titration experiment to determine if the simulated patient is a responder.19
Debrief items for this module include discussion of which modes are appropriate for serving the goal of safety, interpretation of capnograms, implications of prolonged time constants, best ventilator adjustments to decrease PEEPauto, and theory of PEEP titration to reduce PEEPauto.
ARDS
The simulated patient is passive throughout the module. For scenario 1, the learners determine the goal, select the mode, and adjust the settings. Scenario 2 focuses on appropriate selection of PEEP and FIO2 using ARDS Network tables.20 During scenarios 3 and 4, learners select a strategy to deal with hypoxia and decide how to optimize ventilator settings.
Debrief items of this module include discussion of the objectives of the safety goal, appropriate modes and settings, how to read a PEEP-FIO2 table (eg, interpolating PEEP values for FIO2 increments of 0.05 instead of 0.10), Pplat measurement and interpretation, and recruitment procedures.
SEVA-master
SEVA-master takes place at a simulation center and uses standard and custom-built manikins as well as state-of-the-art breathing simulators and ventilators. Participants learn about advanced monitoring techniques. This is the final course that brings learners to the mastery level by training them on specialized procedures in a simulation center environment. Upon completion of SEVA-master, learners are presented with a certificate and a SEVA lapel pin.
Learners in teams of 2–6 rotate between 6 stations to learn the following skills:
Esophageal Pressure Monitoring
This module begins with a slide show that introduces the concepts of esophageal pressure monitoring. Learners practice adjusting the position of an esophageal pressure catheter in a specially constructed manikin. Procedures are taught for connecting the catheter to either a ventilator with esophageal pressure monitoring capability or to a standard hemodynamic monitor (substituting esophageal pressure for the blood pressure signal). Esophageal pressure is used to calculate transpulmonary pressure, which is then used in calculations to optimize VT and PEEP.
Work of Breathing
This module begins with a slide show that introduces the concepts of mechanical work and power as they relate to mechanical ventilation. Because ventilators do not yet monitor these variables, alternative variables are described including airway-occlusion pressure (P0.1) and tidal pressure (also known as, driving pressure or ΔP = VT/C). For the practice portion of this module, a breathing simulator connected to a ventilator is used to represent patients with normal, ARDS, and COPD physiology and different inspiratory efforts. Learners are asked to record VT, Pplat, PEEPtotal, P0.1, and ΔP. Then they are asked to interpret their findings. Emphasis is placed on correct calculation of ΔP using PEEPtot instead of set PEEP.13
Optimum Tidal Volume and PEEP
This module begins with a slide show that introduces the concepts of pressure-volume curves and recruitment maneuvers, including a discussion of the stress index. For the practice portion of this module, learners use the Hamilton-C6 patient-ventilator simulator (https://hamilton-c6.en.aptoide.com/app) to practice recruitment maneuvers with the P/V Tool.
Volumetric Capnography
This module begins with a slide show that introduces the concepts of volumetric capnography. The practice portion of the module shows learners how to use stand-alone monitors as well as capnography features of some ventilators (eg, Getinge Servo-u and Hamilton-C6).
Liberation From Ventilation
This module begins with a slide show that introduces the concepts of how to liberate the patient from mechanical ventilation. The practice portion of the module has 3 scenarios using a breathing simulator. Scenario 1 is an elderly patient with COPD being ventilated but awake and alert. Learners are asked to decide if a spontaneous breathing trial (SBT) is indicated and if so initiate it and interpret the results. Scenario 2 is a patient with ARDS who has passed a spontaneous awakening trial. Learners are asked to start an SBT (which the simulator is programed to make the simulated patient fail). Scenario 3 is a patient on pressure support with an order for a T-piece trial. Learners are instructed on equipment assembly and initiation of the SBT. Debrief items for this module include SBT pass/fail criteria, selection of ventilator settings for SBT, and use and misuse of the rapid shallow breathing index.21
Advanced Modes of Ventilation
This module begins with a slide show that explains 2 advanced modes of mechanical ventilation: NAVA and ASV. Learners discover how ASV makes automatic adjustments as the patient’s respiratory system mechanics (R, C, and Pmus) change. For demonstrating NAVA, we have discovered that if you tape a neonatal NAVA catheter to the instructor’s arm flexing the forearm muscles will produce a realistic EAdi signal that can be used to demonstrate how NAVA adjusts inspiratory pressure in proportion to inspiratory effort. For both modes, the theory of increasing and decreasing support is explained and demonstrated.
SEVA Resources
The SEVA education program has led to several major spin-off projects: SEVA-VentRounds, the Ventilator Mode Map smartphone application, and modifications to our electronic health care record system (Epic).
SEVA-VentRounds
SEVA-VentRounds is a biweekly, online, interactive discussion led by our ICU director, Dr Mireles-Cabodevila, and me (Fig. 16). Here we review basic SEVA concepts and analyze actual screenshots from ventilators in the ICU. The formant is a formal 3-step process to analyze PVI problems. The idea is to identify the mode, the primary abnormality (resistance, compliance, inspiratory effort), and then a thorough analysis of any patient-ventilator synchrony issues. This procedure has been described in detail elsewhere.8 VentRounds is open to the public, and we have clinicians from all over the world participating. Viewers are encouraged to send in their unique screenshots for analysis.

SEVA-VentRounds is a biweekly, online, interactive discussion focusing on waveform interpretation.
Smartphone App
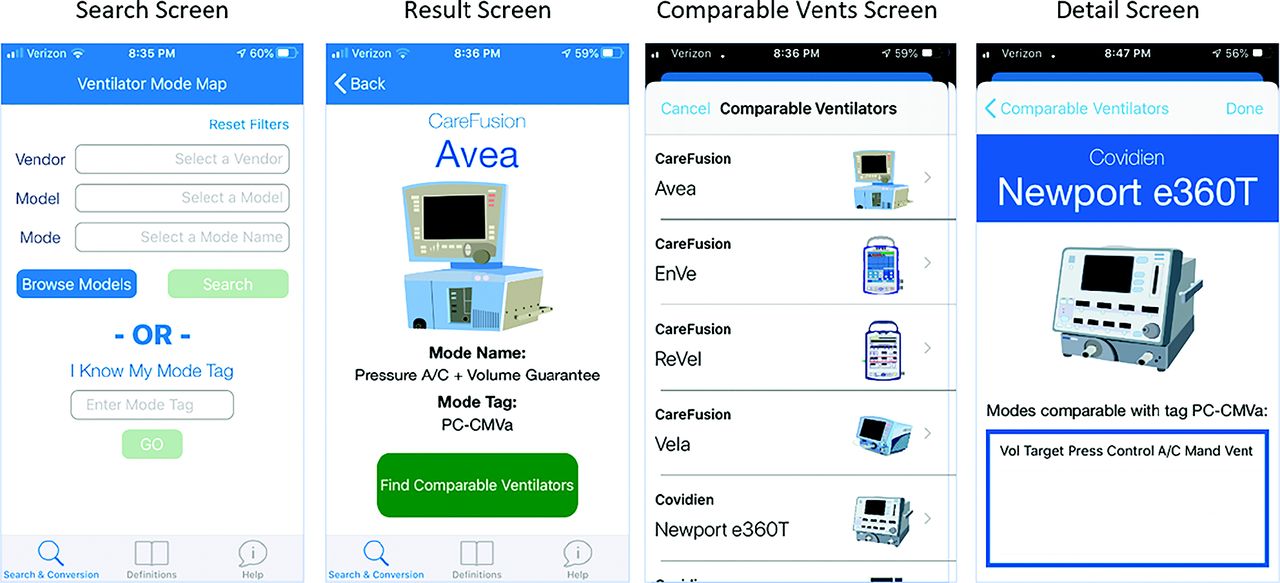
We have developed a free smartphone app that is a database that names and classifies all the modes on virtually all of the ventilators used in the United States (Fig. 17). This is an essential tool for comparing modes on different ventilators and is helpful at the bedside as well as when attending SEVA-VentRounds.

Ventilator Mode Map is a free smartphone application for Android and iOS. Reproduced with permission from Cleveland Clinic.
Electronic Medical Records
Our hospital uses Epic for the electronic health care record system. In Epic, drugs are ordered by generic name with brand names in parentheses (Fig. 18). We have modified Epic so that ventilator orders can be entered and reviewed in a similar way (Fig. 19). Notice that any orders for specific mode settings are entered using context-sensitive menus so that only the settings relevant to the ordered mode are presented. This speeds order entry and avoids confusion. This approach has also been adopted at Cincinnati Children’s Hospital Medical Center as described in a recent publication. That paper concluded that “The proposed framework standardizes mechanical ventilation terminology and may facilitate efficient data exchange in a multisite network. Rapid data sharing is necessary to improve research and clinical care for children with long term mechanical ventilator dependence.”22 Naturally, these benefits extend to all patients. RTs subsequently enter the mode and settings into specific patients’ charts using the same approach (Fig. 20).

Epic drug order screen (fictitious patient) showing generic drug name and brand name in parentheses.

Epic ventilator order screen and order review screen.

Patient charting screen showing a drop-down menu for entering the mode on the right.
Assuring Ongoing Competency
It is one thing to provide advanced learning experiences. But assuring ongoing competency is another matter altogether. The goal of SEVA training is behavior change and ultimately improved patient care. To sustain the educational advances of the SEVA program, we have developed a “gamified” system to maintain competency.
SEVA-challenge
Once a week we send out e-mails to all the respiratory care staff, with a QR code linked to MyLearning. There they will find an image of a real ventilator screen taken from a real patient during routine mechanical ventilation (from the collection of Ariel Garnero). Along with the image are several multiple-choice questions in the same format as SEVA-VentRounds (Fig. 21). Participants who return perfect scores are publicly declared the winners. Our main campus education coordinator manages the program and awards small gifts to the winners (eg, T-shirts, cups, or tote bags, all imprinted with the EoM).

Example of a weekly SEVA-challenge.
Adaptive Learning Support
We have partnered with OttoLearn, an adaptive learning platform, to reinforce our training program and keep knowledge retention within a set mastery level standard (https://www.ottolearn.com). OttoLearn is designed to address 2 key challenges in organizational training:
(1) low learner engagement
(2) poor knowledge retention
It uses the latest cognitive science theories including gamification, deep encoding, and adaptive training. Learners engage with short, personalized training experiences on their phones or computers. We developed OttoLearn content by mapping our existing SEVA course content and optimizing it for adaptive learning.
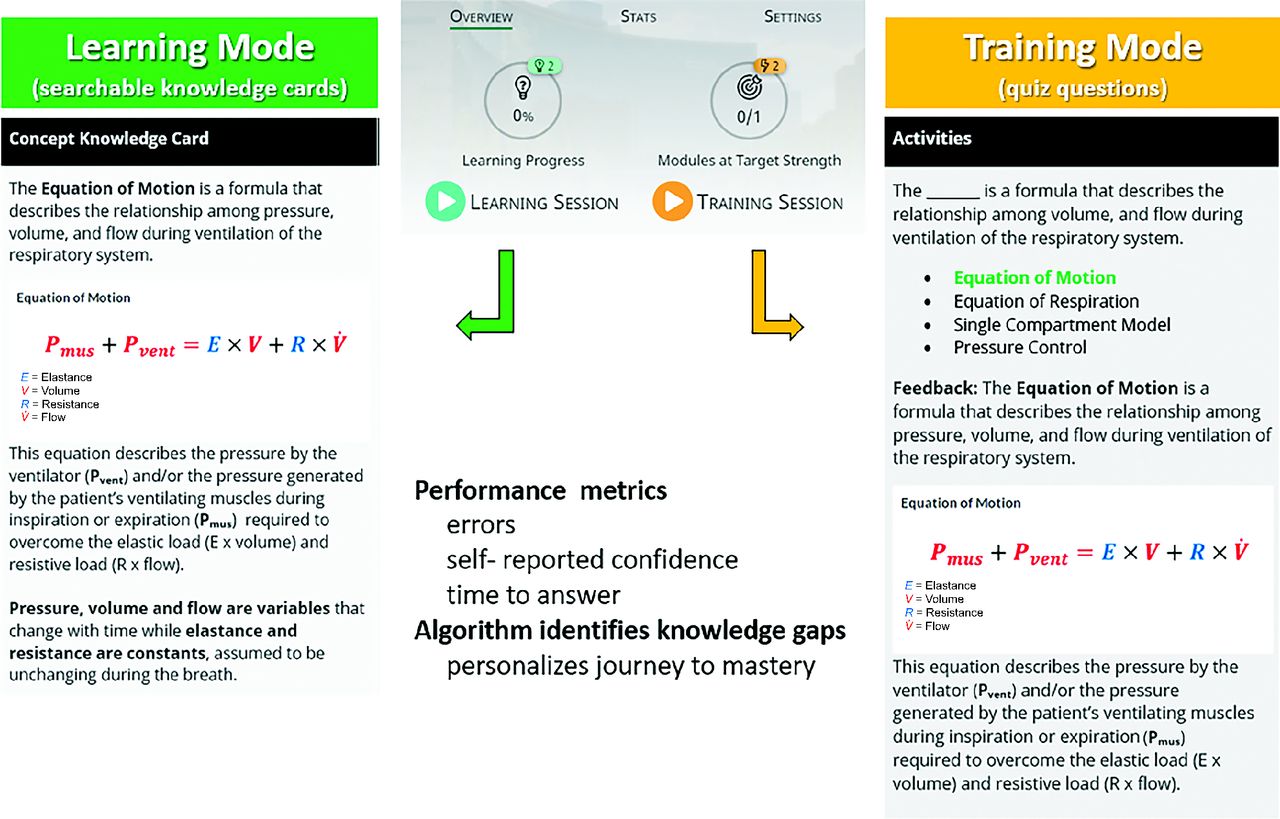
OttoLearn features 2 modes: learning and training (Fig. 22). In the Learning mode, users are directed to complete sessions where they are presented with searchable Knowledge Cards that feature long-form content including text, images, and other forms of media. In the Training mode, users are proactively nudged and presented with contextual activity questions for which they can earn points. These points can then be redeemed for various rewards and benefits. Performance metrics are recorded based on errors, self-reported confidence levels, and time to answer. A proprietary algorithm uses these data to identify knowledge gaps and then personalizes the training journey to mastery.

The OttoLearn platform.
OttoLearn provides detailed analytics in multiple report formats. We are able to see which learners are participating, which learners are in mastery, and which learners are struggling and may require a few short training sessions to get back into mastery on a given topic.
Summary
A wise man once said that any sufficiently complex technology is useless without a taxonomy. More to the point, any such technology is useless without a practical means of teaching it to clinicians beyond simple classification of domain concepts. Such is the state of general education for mechanical ventilation at present. The medical profession is in dire need of a standardized approach to teaching and learning this subject. That need has been voiced by the AARC 2015 and Beyond project1,2 and demonstrated by the recent COVID-19 pandemic. This paper is an introduction to one path toward satisfying that need.
Footnotes
- Correspondence: Robert L Chatburn MHHS RRT RRT-NPS FAARC. E-mail: chatbur{at}CCF.org
Mr Chatburn discloses relationships with IngMar, Vyaire, Timpel, Inovytec, Aires, Ventis, Promedic, and AutoMedx.
Mr Chatburn presented a version of this paper as the Robert M Kacmarek Scientific Memorial Lecture at AARC Congress 2022, held November 9–12, 2022, in New Orleans, Louisiana.
Supplementary material related to this paper is available at http://www.rcjournal.com.
- Copyright © 2023 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}