

Abstract
BACKGROUND: Positive expiratory pressure (PEP) is used for airway clearance in cystic fibrosis (CF) patients. Hypertonic saline (HTS) aerosol increases sputum expectoration volume and may improve respiratory secretion properties. CPAP may also be used to maintain airway patency and mobilize secretions. To evaluate if CPAP would increase the beneficial clearance effect of HTS in subjects with CF, we investigated the effects of CPAP alone and CPAP followed by HTS on sputum physical properties and expectoration volume in CF subjects.
METHODS: In this crossover study, 15 CF subjects (mean age 19 y old) were randomized to interventions, 48 hours apart: directed coughs (control), CPAP at 10 cm H2O, HTS 7%, and both CPAP and HTS (CPAP+HTS). Sputum collection was performed at baseline and after interventions. Expectorated volume was determined and in vitro sputum properties were analyzed for contact angle and cough clearability.
RESULTS: There were no significant differences between any treatment in arterial blood pressure, heart rate, or pulse oximetry, between the 2 time points. HTS and CPAP+HTS improved cough clearability by 50% (P = .001) and expectorated volume secretion by 530% (P = .001). However, there were no differences between control and CPAP on sputum contact angle, cough clearability, or volume of expectorated secretion.
CONCLUSIONS: CPAP alone had no effect on mucus clearance, sputum properties, or expectorated volume, and did not potentiate the effect of HTS alone in CF subjects.
Introduction
Persons with cystic fibrosis (CF) have defective airway ion and water secretion that may result in altered mucus clearance.1,2 Standard treatment for CF patients includes physiotherapy and medications to improve sputum clearance.3–5 Positive expiratory pressure (PEP) mask therapy has been successfully used for airway clearance in CF patients.6 PEP increases intrathoracic pressure and functional residual capacity, with improvement in collateral ventilation. CPAP is a treatment used in patients with respiratory impairment to decrease dyspnea7 and improve respiratory muscle function.8 Application of positive pressure increases tidal volume and reduces the respiratory rate.9 Theoretically, CPAP may help mobilize secretions by minimizing dynamic airway collapse that would decrease atelectasis, increase lung volume, and increase peak expiratory cough flow, similarly to PEP.10,11
To our knowledge, there are no data on the effects of CPAP alone on mucus clearance in CF. We wished to evaluate if CPAP would increase the effect of hypertonic saline (HTS) on sputum properties or expectorated volume in subjects with CF.12–14 HTS is a treatment that facilitates airway clearance in CF by hydrating the airways,15 and since CPAP would mobilize secretions, the 2 treatments could by synergism improve sputum clearance. In this study we evaluated the effects of CPAP alone and CPAP followed by HTS on mucus clearance, sputum physical properties, and expectoration volume in persons with CF.
QUICK LOOK
Current knowledge
Aerosolized hypertonic saline and CPAP are both used to improve secretion mobilization in patients with cystic fibrosis. The combination of hypertonic saline aerosol and CPAP has not been evaluated.
What this paper contributes to our knowledge
CPAP alone had no effect on mucus clearance, sputum properties, or expectorated sputum volume, and did not potentiate the effect of hypertonic saline alone in patients with cystic fibrosis.
Methods
Subjects
This crossover study was approved by the Cystic Fibrosis Association of Belo Horizonte, Minas Gerais, and by the ethics committee of Universidade Cidade de São Paulo, Sao Paulo, Brazil. Written informed consent was obtained from subjects ages ≥ 18 years, and from parents of younger subjects.
We invited subjects listed by the CF Association of Belo Horizonte, Minas Gerais, who were > 8 years old. We excluded subjects who were smokers, those with difficulty completing study procedures, and patients with chronic respiratory infection with Burkholderia cepacia. There is evidence that this strain is more transmissible than others, and the local recommendation is to avoid cross-infection risk. Subjects were also excluded from the study if they had 4 or more clinical signs or symptoms of an acute respiratory exacerbation, including changes in sputum production, new or increased hemoptysis, increased cough, increased dyspnea, malaise, fatigue or lethargy, fever, anorexia or weight loss, sinus pain or tenderness, changes in nasal discharge, loss of appetite, or > 10% deterioration in lung function during the study period.16
Study Protocol
After inclusion, pulmonary function was measured (Microlab 3500, Micro Medical, Rochester, United Kingdom) using American Thoracic Society guidelines17 to determine FEV1 and FVC as percentages of predicted values and the absolute values of FEV1/FVC.18
All subjects continued their regular, prescribed, individualized treatment regimen, except that bronchodilators and dornase alfa (Pulmozyme, Genentech, South San Francisco, California) were discontinued for 24 hours before each study visit in order to minimize confounding variables, and the normal airway clearance in the morning of the study visit was withheld and replaced by one of the specified treatments. Each subject participated in 4 visits, conducted 48 hours apart, between 8 am and noon. Each subject performed one intervention in the randomly selected order at each visit. Randomization with sealed cards was used to determine intervention order. Directed cough was standardized as a series of 3 coughs on command and used as the control intervention. CPAP at 10 cm H2O delivered through a face mask (Sullivan Comfort System, ResMed, San Diego, California) for 30 min. CPAP+HTS was 30 min of CPAP at 10 cm H2O, followed by inhalation of HTS 7% delivered by a jet nebulizer (Proneb Ultra II or LC Plus Pari Respiratory Equipment, Midlothian, Virginia) over 15 min (total time of 45 min). HTS alone was inhalation of HTS over 15 min.
At each study visit, subjects were asked to rest in a sitting position for 15 min. Heart rate, arterial blood pressure, and respiratory rate were measured immediately before (baseline) and after a random intervention. Subjects were asked to rinse their mouth first (and after inhalation of HTS), and then cough 3 times to measure baseline sputum properties and volume.
Sputum Volume
Subjects were asked to rinse their mouth, gargle, and expectorate sputum samples. Sputum was visually separated from saliva and immediately stored in sealed plastic tubes.19 Expectorated secretion volume was visually measured from the container, which was graduated from 0.1 mL to 2.0 mL, and confirmed by 2 investigators who were blinded to the interventions. After volume measurement, samples were stored at −70°C until analyzed for cough clearability and contact angle, as detailed below.
In Vitro Sputum Cough Clearability
We used a simulated cough machine to measure in vitro cough clearability.20 This device reproduces the flow and time pattern of a natural cough. Cough clearability was determined by measuring the distance traveled by 25 μL of sputum after a single air flow burst in an artificial trachea. Air is pressurized at 40 psi in a tank, and the simulated “cough” is initiated by a solenoid valve releasing the air into an acrylic tube with inner diameter of 4 mm and a length of 133 mm.20,21 Three tests were run with each sample, and the results were averaged.
Wettability by Contact Angle
Contact angle characterizes the surface wettability, or the ability of a fluid to spread as a sessile drop when deposited on a solid planar surface.21,22 The contact angle was measured by using a camera (AxioCam, Carl Zeiss, Oberkochen, Germany) and interactive software (Axiovision 4.7.1, Carl Zeiss, Oberkochen, Germany), as previously described.23 Briefly, 25 μL of sputum was dropped on a glass plate, pretreated with sulfochromic acid solution to remove electrostatic charge. Contact angle results of sputum sample were expressed in degrees as the average of 3 measurements.
Statistical Analysis
Statistical analyses were carried out using statistics software SPSS 17, SPSS, Chicago, Illinois). When normally distributed, data are expressed as mean values and 95% CI, or as median (interquartile range [IQR]) when appropriate. Comparisons between interventions over time were analyzed using analysis of variance for repeated measures, with post-hoc comparisons conducted with Tukey test or by Friedman test. P < .05 (2-tailed) was considered to be statistically significant.
Results
Seventeen subjects (11 male) entered into the study. Two female subjects were excluded from study analysis due to exacerbation of the disease during the study period. Therefore 15 subjects completed the study, with a mean age of 19 years (range 8–33 y), a mean sweat chloride concentration of 108.8 mEq/L (95% CI 97.3–120.3 mEq/L), and mean body mass index of 17.4 kg/m2 (95% CI 15.9–19.0 kg/m2). Pulmonary function testing showed a mean percent-of-predicted FEV1 of 53.5% (95% CI 43.7–63.4%) and a mean percent-of-predicted FVC of 70.3% (95% CI 62.1–78.6%). There were no significant differences after any treatment in arterial blood pressure, heart rate, respiratory rate, or pulse oximetry (data not shown). One CF subject presented bronchospasm with HTS alone, and this subject was treated with salbutamol (albuterol).
Sputum Volume and Physical Properties
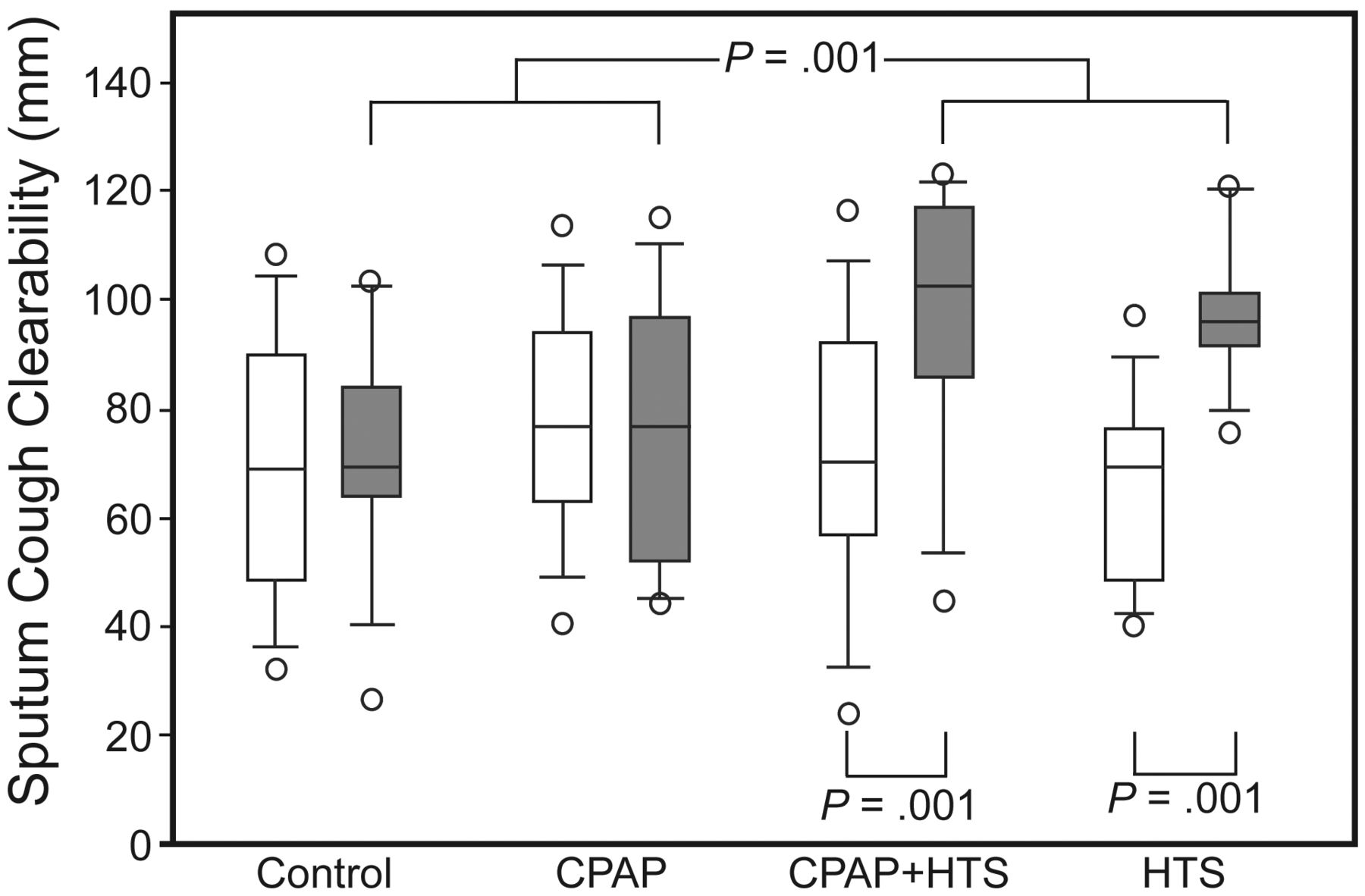
There were no differences in sputum contact angle at baseline or after any intervention (Table). No differences were found between HTS and CPAP+HTS or between control and CPAP on in vitro cough clearability or sputum volume. However, HTS and CPAP+HTS increased sputum volume by 5-fold (P = .001) and in vitro cough clearability by 50% (P = .001) compared with control or CPAP (Figs. 1 and 2).
Sputum Volume, Cough Clearability, and Contact Angle

In vitro sputum cough clearability after directed coughs (control), CPAP, CPAP combined with inhalation of hypertonic saline aerosol (CPAP+HTS), or inhalation of HTS alone in 15 CF subjects. Significant differences were observed after HTS and CPAP+HTS interventions, compared with baseline and compared with control and CPAP.

Sputum volume after control (directed coughs), CPAP, CPAP plus hypertonic saline (HTS), and HTS alone.
Discussion
Therapy that improves the clearance of respiratory secretions is important in the routine care of CF patients. In this study we investigated the effects of CPAP by itself and CPAP followed by HTS, compared with coughs and HTS alone, on sputum properties and expectorated sputum volume. HTS significantly increased expectorated sputum volume and sputum in vitro cough clearability. Unlike PEP therapy,6 CPAP alone had no effect on mucus clearance, sputum properties, or expectorated volume, and CPAP did not potentiate the HTS effects.
Mucus is the first barrier in the defense of the airways against microorganisms. In the CF airways there appear to be decreased airway surface liquid and increased DNA/F-actin polymers mixed with inflammatory cells, cellular debris, and bacteria, which compromise mucociliary and cough clearance.5,15,24,25 HTS is a mucoactive agent that is well tolerated.12,13,15 HTS is thought to transiently improve airway surface liquid volume and promote effective cough.5,12,13,22 HTS improves pulmonary function in CF,12 increases expectorated sputum volume,13 and decreases the frequency of respiratory exacerbations.15 In the current study, HTS improved mucus clearance by cough, as observed by the robust increase in expectorated sputum volume. Additionally, HTS improved in vitro sputum cough clearability by 50%, with no changes in sputum contact angle. Cough clearability is determined by the sputum surface properties, and the surface interaction between mucus and the epithelium.5,13,26 HTS may have decreased tenacity (the product of adhesivity and cohesivity), which has been shown to be the primary determinant of sputum cough clearability in vitro.27 Only one subject had evidence of bronchospasm with HTS alone, and this subject was treated with salbutamol. However, the results on sputum properties or on expectorated volume were not changed by including or excluding this single subject.
Noninvasive mechanical ventilation has been used to treat respiratory failure and has been used as a bridge to lung transplantation in CF.28,29 CPAP maintains constant airway pressure during inspiration and exhalation, decreasing dynamic airway closure, airway resistance, respiratory muscle work load, and oxygen consumption. We tested CPAP at 10 cm H2O, a level shown to be comfortable for patients with severe CF.28,29 Although CPAP has primarily been used in subjects with lung disease more severe than those in this study, persons with mild to moderately compromised lung function can also have low cough flow.30 Theoretically, the use of CPAP alone could improve secretion clearance in CF by decreasing dynamic airway collapse and enhancing aerosol deposition.10,11 However, we found no effects of mask CPAP alone on mucus clearance, sputum cough clearability, or the volume of expectorated sputum, and no additive effects of CPAP when followed by HTS inhalation. We were not particularly surprised to see these results, but pleased that CPAP did not decrease sputum expectoration in these subjects with moderately severe CF lung disease.
This study found large and robust effects of HTS on cough clearability and the volume of expectorated secretion, compared with the other 2 interventions (control and CPAP). One could argue that the volume of expectorated sputum may have been affected by the differences in period of time between interventions, since the longer time allows more sputum to be collected. However, interventions with HTS alone lasted 15 min, and the time of CPAP with HTS was 45 min, with similar increase in expectorated mucus volume. We did not measure changes in pulmonary function or gas trapping with the use of CPAP. However, these subjects were relatively young, with moderately severe lung compromise, pulse oximetry remained stable, and there were no reports or signs of respiratory discomfort. In the present study, CPAP was not simultaneously applied with HTS, but was administered before HTS inhalation. First, there are few studies that have assessed the ability to give inhaled medications during noninvasive mechanical ventilation,31–33 and very few with CPAP.34 HTS has a hygroscopic growth characteristic that increases the droplet particle size and leads to a predominant central lung deposition with low lung penetration capability, even with small HTS particle size.35 In a bench study of the simultaneous application of CPAP with salbutamol inhalation, a decrease rather than an increase in lung deposition of the bronchodilator has been reported with the use of old masks with large inspiratory and expiratory ports.34 A recent study showed that simultaneous application of HTS and PEP nebulizer induces functional and tolerance improvement in CF subjects.36 However, they were not able to separate the effects of HTS and PEP nebulizer.
Conclusions
Our findings suggest that CPAP alone does not improve sputum clearance nor does it appear to augment the effect of HTS in subjects with mild to moderately severe CF. HTS markedly improved mucus clearance by cough.
Acknowledgments
The authors would like to thank Dr Julia Fukushima for helping us with the statistical analysis.
Footnotes
- Correspondence: Naomi Kondo Nakagawa MSc PhD, Department of Physiotherapy, Communication Science and Disorders, and Occupational Therapy, Laboratório de Investigação Médica 34, Faculdade de Medicina da Universidade de São Paulo, Brazil. Avenida Doutor Arnaldo 455, Room 1150, Cerqueira Cesar, São Paulo, Brazil 01246–903. E-mail: naomi.kondo{at}usp.br.
This research was partly supported by grant 07/51605–9 from Fundação de Amparo à Pesquisa do Estado de São Paulo.
The authors have disclosed no conflicts of interest.
- Copyright © 2012 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}