

Abstract
BACKGROUND: Chest x-ray (CXR) is widely used for diagnosing and screening pulmonary tuberculosis (PTB), yet its validity is debatable and its costs are relatively high. This study aimed to determine the validity of CXR screening in detecting radiological findings compatible with active PTB or with old healed tuberculosis (OHTB).
METHODS: All Ethiopian immigrants to Israel between 2001 and 2005 were radiographed before emigration. Immigrants whose CXR demonstrated PTB or OHTB were evaluated, treated, and followed for one year after arrival. The end point of this historical cohort study was a diagnosis of active pulmonary disease within the study period.
RESULTS: CXR was performed on 13,379 immigrants. Changes suggesting PTB were identified in 150 (1.1%) of those, and 46 were diagnosed with active PTB. Sensitivity, specificity, and positive predictive value of a CXR suggesting PTB were 80.1%, 99.2%, and 31%, respectively. As PTB prevalence in this cohort is 0.4%, post-test odds for CXR suggestive of PTB were 75.5. Changes suggesting OHTB were identified in 257 (1.9%) immigrants. Of those, 15 (5.8%) developed active PTB within one year following arrival. Sensitivity, specificity, and positive predictive value of CXR suggestive of OHTB were 17.2%, 98.2%, and 5.8%, respectively, when active PTB during the first year was the end point. In this study, 291 CXR were required to detect one active PTB patient, costing $5,802.
CONCLUSIONS: CXR is a valid and cost-saving tool for screening active PTB in immigrants originating in high-burden countries, and is beneficial in detecting OHTB in immigrants who are at a higher risk for developing active PTB.
Introduction
The total number of new cases of tuberculosis in developed countries has declined since the second half of the 1990s. Nevertheless, the proportion of tuberculosis in immigrants originating from high-burden countries relative to all tuberculosis cases reported has increased.1–3 Immigrant screening for tuberculosis is a standard policy in many developed countries,4 and one of the screening tools that is widely used for diagnosing pulmonary tuberculosis (PTB) remains chest x-ray (CXR).5 Its reliability depends on the readers' experience,6 their knowledge of the human immunodeficiency virus (HIV) status of the patient, and the quality of the film.7 The World Health Organization reserves CXR for the diagnosis of tuberculosis for suspects with negative smears, and recommends symptoms questionnaire or sputum smear for screening,8,9 due to the low specificity of CXR, leading to a 37% over-diagnosis.10
Radiographic imaging of calcifications or fibrosis may be indicative of latent tuberculosis infection (LTBI).11 Some studies have found CXR to be a cost-effective screening tool for detecting LTBI,3,12 while others failed to reproduce those findings.13
Screening Procedure
Every person of Jewish ancestry is granted the right to immigrate to Israel.14 These immigrants are naturalized upon arrival and are medically insured by the National Insurance Law. Ethiopia has a higher incidence of tuberculosis, compared to Israel, with an estimated incidence of 344 cases per 100,000 populations in 2005, whereas in Israel 8 cases per 100,000 were notified during the same period.15 All Jewish Ethiopian immigrants to Israel are screened for PTB in Addis Ababa since June 2001, including CXR for all non-pregnant immigrants older than one year, using the postero-anterior aspect 2–3 weeks before air-travel.16 To ensure consistency, all films are read by the radiography department in Carmel Hospital in Haifa, Israel. Each immigrant also completes a symptoms questionnaire (screened immigrants were asked to respond whether they suffered from prolonged cough, lasting > 3 weeks, hemoptysis, chest pain, fever [> 38°C], night sweats, and weight loss), and undergoes physical examination and a one-step tuberculin skin test (TST). Individuals who had previously been treated for tuberculosis have a positive response in the symptoms questionnaire, and those whose CXR shows changes suggestive of PTB are also asked to provide sputum samples on 3 consecutive days for smear and culture. PTB patients are treated in Ethiopia by directly observed therapy, which is later resumed in Israel.
Upon arrival, Ethiopian immigrants are housed in spacious absorption centers for periods longer than a year. A public-health nurse visits the immigrants within a week, collects blood samples for HIV, and performs a second-step TST in individuals whose first step shows indurations < 10 mm. Individuals complaining of tuberculosis symptoms or showing positive findings on either CXR or TST are referred to the regional tuberculosis clinics.17 Immigrants diagnosed with PTB are treated by directly observed therapy, while those with LTBI are recommended isoniazid therapy and are followed up monthly. All otherwise healthy immigrants who demonstrated an unremarkable CXR are followed by a nurse for the first year. Any symptomatic immigrants and contacts of PTB patients are referred to the tuberculosis clinic.
Nevertheless, additional data are essential to define the accuracy of CXR screening among immigrants from high-burden countries, as this information may support the current Israeli policy for tuberculosis screening. We hypothesized that the accuracy of CXR in detecting PTB in mass screening of individuals from high-burden countries justifies the process.
QUICK LOOK
Current knowledge
Chest x-ray (CXR) is widely used for diagnosing and screening for pulmonary tuberculosis (PTB) in immigrant populations from at risk regions. The validity of CXR screening is debatable, and the costs are relatively high.
What this paper contributes to our knowledge
CXR is a valid and cost-saving tool for screening active PTB in immigrants originating in high-burden countries, and is beneficial in detecting old healed tuberculosis in immigrants who are at a higher risk for developing active PTB.
Methods
The clinical diagnoses in this study were performed according to the British Health Protection Agency terms,18 and the radiological findings were based on the criteria set by the American Thoracic Society,19 as performed in Israel.
Clinical Diagnoses
Active PTB.
Symptomatic patient with pulmonary disease and confirmed Mycobacterium tuberculosis complex culture.
Undocumented PTB.
Undocumented PTB was defined when clinical judgment led to a decision to treat the patient with a full course of anti-tuberculous therapy following treatment failure with broad-spectrum antibiotics.20,21
LTBI.
A positive induration to TST (≥ 5 mm for HIV infected individuals, and ≥ 10 mm for all other immigrants without evidence of active PTB).
Old Healed TB.
CXR image compatible with previous tuberculosis disease that had either healed naturally or been fully treated and no radiological finding of current activity.
Radiological Diagnosis
Findings consistent with PTB in CXR included at least one of the following: upper or middle lobe infiltrate, pleural disease without fibrosis, bronchopneumonia, cavitations, consolidation, and hilar/intrathoracic lymphadenopathy, or radiologist comment “suspected TB.” CXR findings compatible with old healed TB (OHTB) included dense nodular opacities with or without calcifications in hilar areas or upper lobes, apical fibrosis or fibrotic scar, granuloma, pleural thickening/plaques, or radiologist comment “old TB.” CXR was reported normal if there was no evidence of pathology pertaining to tuberculosis. Accuracy of CXR was determined by the diagnosis of active PTB using 2 end points as a gold standard for PTB: microbial and clinical. The first end point measures the efficacy and is a statistically pure characteristic of CXR, while the second evaluates the effectiveness of this instrument and may better reflect the “real life” clinical use of CXR, as some areas in developing countries may lack the capacity to perform culture.22
Data Collection
Retrospective records from the Ministries of Health, Immigration, and Interior, from the Jewish Agency and the tuberculosis clinics. The study was approved by the Tel-Aviv University review board.
Data Analysis
Statistics software (SPSS 14.0, SPSS, Chicago, Illinois) was used. Comparisons between groups were made using the chi-square or Fisher exact test for categorical variables, and the Student t test for continuous attributes. All P values reported are based on 2-tailed comparisons, with statistical significance set at P < .05.
The accuracy attributes of CXR were expressed by sensitivity, specificity, positive and negative predictive values (PPV and NPV, respectively), and positive and negative diagnostic likelihood ratios. The latter were calculated as sensitivity/(1 – specificity) and (1 – sensitivity)/specificity, respectively. Pre-test odds were calculated as pre-test probability/(1 – pre-test probability), while post-test odds were calculated as pre-test odds times positive likelihood ratio.
Results
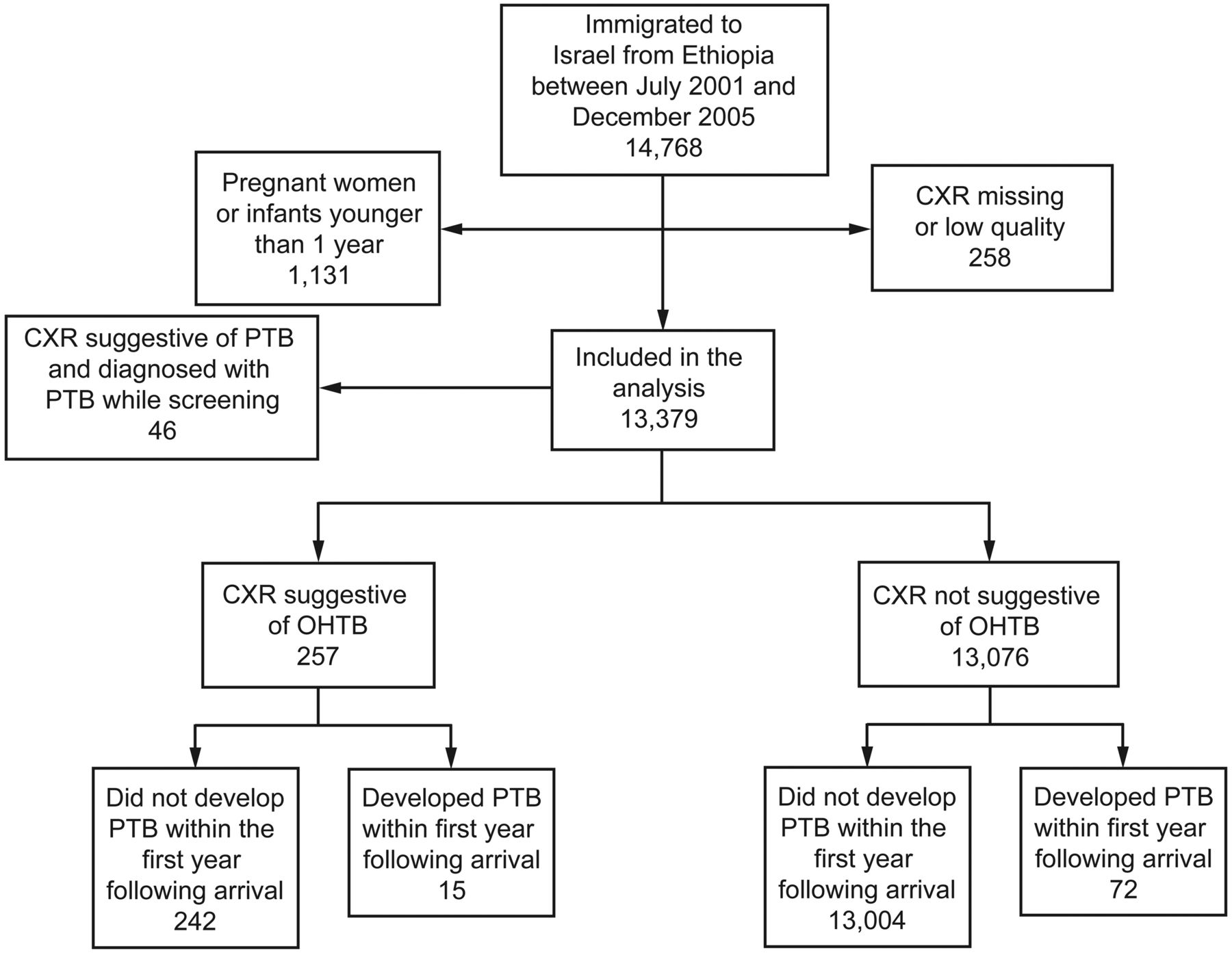
Between July 2001 to December 2005, 14,768 Jewish Ethiopian immigrants arrived in Israel, of whom 13,379 (90.6%) underwent CXR in Ethiopia. The remaining 1,131 were pregnant women or infants younger than one year. PTB was suggested in 150 (1.1%) of films, OHTB was suggested in 257 (1.9%), and 12,972 (97%) films were unremarkable or demonstrated other abnormalities unrelated to tuberculosis (Figs. 1 and 2).
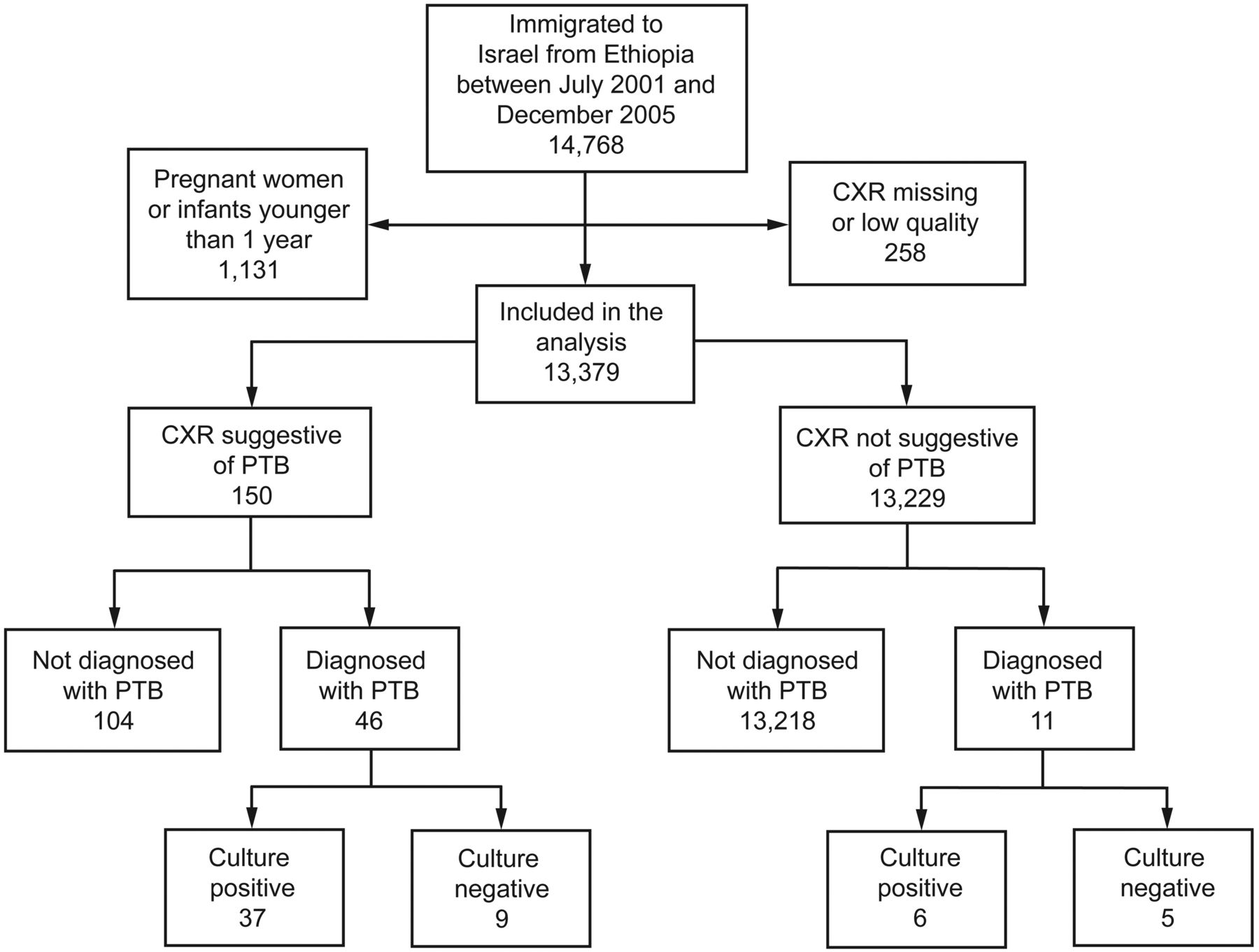
Screening results in diagnosing pulmonary tuberculosis (PTB) in Ethiopia. CXR = chest x-ray.
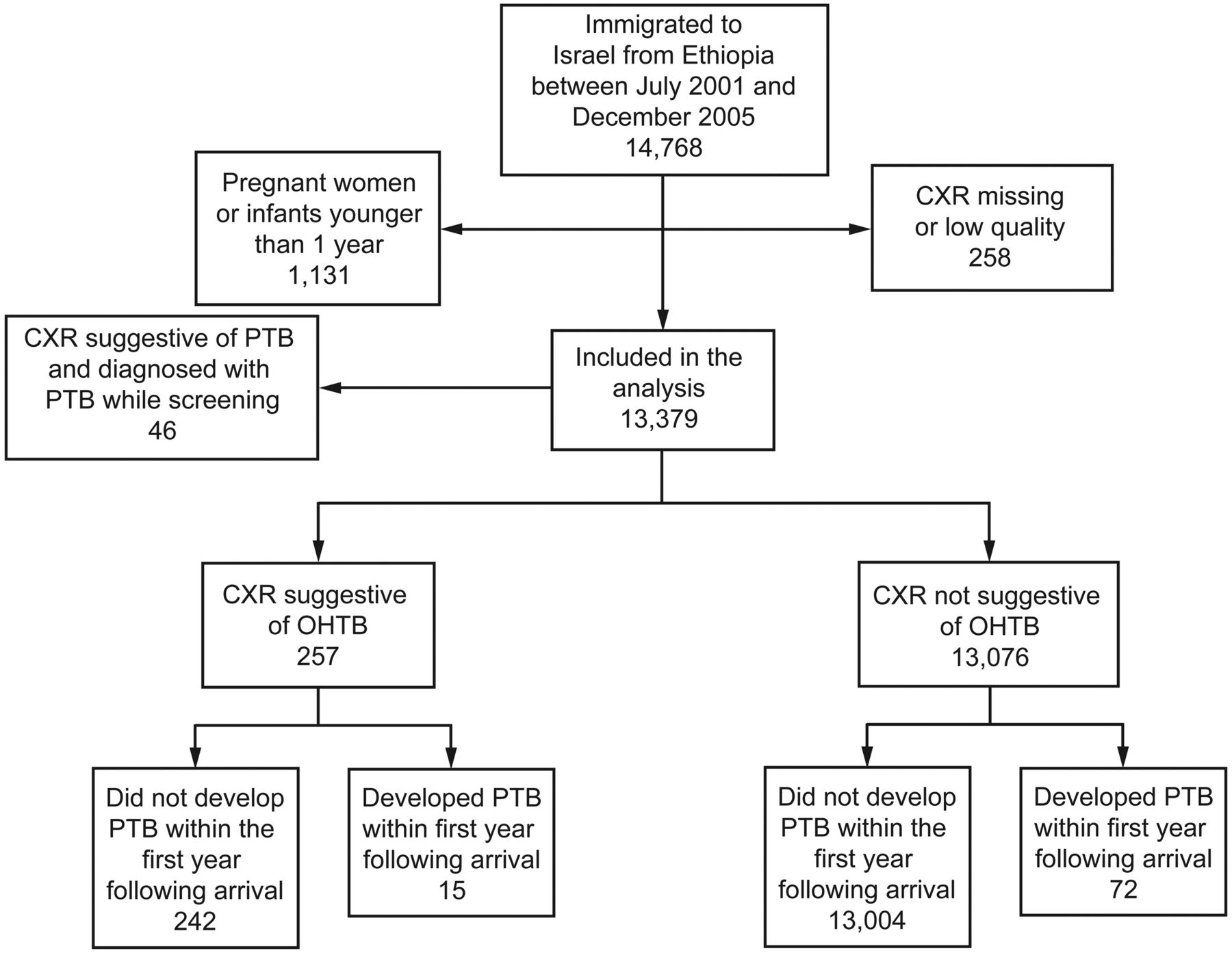
Pulmonary tuberculosis (PTB) diagnosis within one year of follow-up of Ethiopian cohort in Israel after arrival. CXR = chest x-ray. OHTB = old healed tuberculosis.
PTB Diagnosis During Screening
Of all immigrants screened in Ethiopia, 57 (0.4%) were diagnosed with active PTB, including the undocumented cases. Of those, 46 (81%) had a CXR suggestive of PTB, and 11 (19%) patients had an unremarkable CXR. The latter were positively diagnosed following clinical suspicion while responding to the symptoms questionnaire and were smear and/or culture confirmed. Five PTB patients had negative cultures and unremarkable CXR. In comparison to immigrants diagnosed with active PTB and whose CXR was suggestive of PTB, those who were diagnosed with PTB and whose CXR was not suggestive for PTB were relatively older and included a greater percentage of females (Table 1). Only 3 (3.3%) of the active PTB patients had concomitant HIV infection, of those 2 had a CXR suggestive of PTB, one had a positive smear, 2 were contacts of a known patient, and 2 had been previously treated for PTB.
Characteristics of Patients With Pulmonary Tuberculosis Detected During Screening in Ethiopia, by Radiological Evidence of Chest X-Ray
Accuracy of CXR
Of all 13,379 immigrants radiographed, CXR abnormalities consistent with PTB were detected in 150 (1.1%) immigrants, and their sputum was cultured. Of those, in 46 (31%) a clinical diagnosis of active PTB was made, while microbial confirmation was obtained in 37 patients. The sensitivity of CXR as a screening tool for clinical detection of PTB was 80.1% (95% CI 68.1–89.9%), the specificity was 99.2% (95% CI 99.1–99.4%), the PPV was 31% (95% CI 23.4–38.7%), and the NPV was 99.9% (95% CI 99.8–99.95%) (Table 2). The sensitivity of CXR as a screening tool for microbial detection of PTB was 86.1% (95% CI 72.1–94.7%), the specificity was 99.1% (95% CI 99.0–99.3%), the PPV was 24.7% (95% CI 18.0–32.4%), and the NPV was 99.9% (95% CI 99.92–99.99%) (Table 3).
Chest Radiography Suggestive of PTB and PTB Diagnosis (Both Active PTB and Undocumented Cases) of Immigrants Screened in Ethiopia
Chest Radiography Suggestive of PTB and PTB Diagnosis (Bacterial Confirmation) of Immigrants Screened in Ethiopia
The positive diagnostic likelihood ratio for a CXR suggestive of PTB was 100.1 (the probability of an immigrant whose CXR is suggestive of PTB to be diagnosed with active PTB is 100 times greater than those who CXR is unremarkable). In contrast, the negative diagnostic likelihood ratio was 0.2 (unremarkable CXR is 5 times more common in healthy immigrants than in those who developed active PTB).
PTB pre-test probability of this cohort was 0.43% (57/13,379), pre-test odds were 0.75 and the post-test odds for CXR suggestive of PTB were 75.5. These calculations represent a more accurate estimation of the yield of CXR in a “real life” setting, meaning that an Ethiopian immigrant whose CXR demonstrates changes suggestive of PTB is > 75 times more likely to be diagnosed with PTB than an immigrant whose CXR is unremarkable.
Findings suggestive of OHTB in CXR were detected in 257 (1.9%) of all films performed. When the diagnosis of active PTB was ruled out, these immigrants were recommended treatment for LTBI and were followed up. Fifteen (5.8%) of them developed active PTB (culture confirmed) within one year following arrival, representing an incidence rate of 37.3 cases per 100,000 immigrants. None completed the entire treatment course for LTBI. TST records were available for only 8 individuals diagnosed with active PTB (TST results were only marked in the immigrants' personal health cards, and were not routinely available to the tuberculosis clinic nor collected systematically), and therefore the results are not presented. As individuals whose CXR is suggestive of OHTB are at higher risk for developing active PTB, we calculated the diagnostic yield of OHTB-CXR using active PTB diagnosis during the first year following immigration as the end point. Sensitivity was therefore 17.2% (95% CI 10.0–26.9%), specificity was 98.2% (95% CI 97.9–98.4%), and PPV was 5.8% (95% CI 3.31–9.4%) (Table 4). The positive diagnostic likelihood ratio for a CXR suggestive of OHTB was 9.4.
Chest Radiography Suggestive of OHTB and PTB (Bacterial Confirmation) During the First Year in Israel Following Immigration*
Cost of Finding a PTB Case Using CXR Screening
As 46 patients had CXR suggestive of PTB, out of all 13,379 immigrants screened, we calculated that 291 films are required to detect a single case of active PTB upon immigration. The cost of performing a single CXR in Ethiopia, including its reading in Israel, is $20 (including direct cost of CXR in Addis Ababa, reading of CXR in Israel, and indirect costs in Ethiopia, such as maintenance of the health station and salaries). Thus, the total amount required to detect one PTB case among immigrants is $5,820.16
Discussion
The radiological screening for PTB of the 13,379 immigrants yielded a sensitivity of 80.1% and a PPV of 31%. The sensitivity and PPV of CXR demonstrating OHTB as a predictor for developing active PTB during the first year following immigration were significantly lower: 17.2% and 5.8%, respectively.
Although CXR is subject to inter- and intra-observer discrepancies, it is considered a powerful tool for detecting PTB or for ruling-out PTB among individuals with LTBI.10 A literature review of CXR effectiveness in 10 European countries23 showed that CXR detected PTB in a median value of 0.35% of the immigrants, similar to the 0.4% found in our study.
Accuracy of CXR Suggestive of PTB
CXR sensitivity in our study (80.1%) was similar to immigrants screened at the Swiss border,5 but lower than a random sample of tuberculosis out-patient sample performed in Bangalore, India (87.6%),24 or from a sample of tuberculosis suspects in a chest clinic in Nairobi, Kenya (91%).7 CXR sensitivity could be improved by reducing the number of false negative readings, which is expected to occur in 10–43% of the films,10,25 mainly by enhancing the experience and interpretation skills of the radiologists,6 introducing quality control systems, and the introduction of computerized radiography techniques. The rate of false negative results can be reduced if radiologists are privy to the underlying information regarding the immigrant's health, such age, sex, prior tuberculosis disease or therapy, recent contact with tuberculosis patient, and HIV status.
PPV in our study is lower than in the Indian24 and the Kenyan7 studies, but higher than that found in a model based on data from low-burden countries,12 62.5%, 78%, and < 10%, respectively. As PPV is related to the prevalence of the disease in the population examined, the first 2 publications cited examined populations from tuberculosis clinics with higher prevalence than immigrants screened in our study. Physicians should therefore recognize the relatively low PPV of CXR in otherwise healthy immigrants and should be encouraged to use symptoms questionnaire and the clinical history pertaining to tuberculosis and HIV, which increases PPV.26
Children younger than 10 years composed 4 (7%) of all active PTB patients in our study. We perform only a posterior-anterior view CXR, without lateral view,27 and therefore our detection rate in children might be lower than expected. Nevertheless, exclusion of these children from the accuracy calculations did not affect the final results.
Costs of CXR in Detecting PTB
Mass tuberculosis screening for all immigrants is a costly procedure. However, Dasgupta and Menzies12 demonstrated that CXR is more specific and less expensive than skin testing of immigrants originating in high-burden countries. The total costs in their publication for detecting PTB were $9,898 by CXR, and $12,407 by skin test.
The cost of $5,820 for detecting a single case of active PTB in our study was more economical than treating an active PTB patient in Israel, which is $7,619 (based on the Israeli Ministry of Health tariffs in Israel, January 2005).16 The cost of detecting a single case in our study was lower than that reported from Canadian12 or British28 studies: $7,978 and $21,430, respectively.
Nevertheless, one should be aware of false negative rates of up to 20%, mainly in HIV infected individuals,29 as their CXRs may be atypical.30 However, the low HIV prevalence of ∼2% in our cohort16 allows an unbiased assessment of the value of CXR in this cohort.
OHTB as a Predictor of Tuberculosis Reactivation
CXR can be suggestive of radiographic abnormalities compatible with OHTB. These changes were recognized in 257 (1.9%) of all Ethiopian immigrants screened in our study. A rate ratio of 10.6 was found between immigrants in whom CXR indicated OHTB and developed active PTB during the first year, compared to immigrants who developed active PTB but had unremarkable CXR (5,836 and 548 cases per 100,000 immigrants, respectively). This finding is in agreement with the literature, where individuals with radiological evidence of OHTB, especially with fibrotic changes,31 have a 4–6 times greater risk for developing active PTB, compared to individuals with an unremarkable CXR.12,32 A recommendation to treat OHTB cases as LTBI could provide substantial individual and public health benefits and increase the cost-effectiveness of CXR, compared to treating only active and undocumented cases.3
Adherence with treatment for LTBI in our study is unknown, but is considered generally low.33 Better techniques should therefore be employed to increase adherence, to enhance diagnostic accuracy, to augment the treatment efficacy, and to improve the cost-effectiveness of the entire screening process. These could include the administration of treatment of LTBI therapy by directly observed therapy,34 and also shorter courses of chemoprophylaxis.35 Additionally, performing sputum and culture for each immigrant presenting OHTB on CXR may detect active PTB at an earlier stage.
Readers of CXRs should be aware that calcification and fibrosis, which suggest OHTB, may actually represent active PTB.36 Additionally, CXR screening may miss early cases of PTB and may fail to diagnose extra-pulmonary TB.
The findings of this study, using a relatively large cohort of migrants followed up for a year, suggest that CXR is a sensitive and cost saving tool for mass screening. Nevertheless, it may be subject to certain limitations. First, the incomplete access to TST results and the missing clinical symptoms of the immigrants screened weaken the study. However, 13,379 person-years of follow-up allowed a robust retrospective evaluation of CXR interpretation. Consequently, the results of this study are conservative, pertaining purely to CXR results. Second, there was the follow-up period of OHTB patients; yet, the majority of immigrants developed PTB during their first year in Israel following immigration.16 Third, the CXRs were read by several radiologists, so the results are subject to inter-observer differences. In order to minimize over- and under-reporting, all the readings were performed in the same radiology ward, supervised by a single senior physician. Lastly, readers should be aware that PPV is dependent on the prevalence of the disease in the population studied.
Conclusions
CXR is a relatively sensitive and cost-saving tool for mass screening for PTB among immigrants from a high-burden country, as hypothesized. CXR should be considered as a screening tool in developed countries hosting immigrants originating from areas endemic for tuberculosis, so that therapy can be completed.
Acknowledgments
The authors wish to express their gratitude to the following experts. Dr Nira Koren-Morag for her professional biostatistics guidance; Dr Daniel Chemtob, Director of the Department of Tuberculosis and AIDS in the Ministry of Health, for his devoted assistance in data collection; and Mr Zeev Schwartzberg from the Jewish Agency, Ethiopian desk, for his assistance in accessing and organizing the immigrants' documentation. The authors also thank Professor Donald Enarson, senior advisor at International Union Against Tuberculosis and Lung Disease, for reading the paper and providing his beneficial comments.
Footnotes
- Correspondence: Zohar Mor MD, Ministry of Health, 33 Pier Koening Street, PO Box 1176, Jerusalem 91010 Israel. E-mail: zohar.mor{at}rml.health.gov.il.
This study was partially sponsored by the League Against Tuberculosis and Lung Diseases, Rehovot, Israel, and by the National Institute for Health Policy and Health Services Research, Tel-Hashomer, Israel. The authors have disclosed no conflicts of interest.
- Copyright © 2012 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}