

Abstract
BACKGROUND: Little is known about the incidence of and risk factors for adverse effects from endotracheal suctioning. We studied the incidence and risk factors, and evaluated the effect of suctioning practice guidelines.
METHODS: During a 3-month period, in 79 mechanically ventilated subjects, we recorded the adverse effects in 4,506 suctioning procedures. Then practice guidelines were implemented, and 1 year later, during another 3-month period, in 68 subjects, we recorded the adverse effects in 4,994 suctioning procedures.
RESULTS: In the first period, adverse effects occurred frequently: oxygen desaturation in 46.8% of subjects and 6.5% of suctionings, hemorrhagic secretions in 31.6% of subjects and 4% of suctionings, blood pressure change in 24.1% of subjects and 1.6% of suctionings, and heart rate change in 10.1% of subjects and 1.1% of suctionings. After guidelines implementation, all complications, both separately and all together, were reduced. The incidence of all complications together decreased from 59.5% to 42.6% of subjects, and from 12.4% to 4.9% of procedures (both P < .05). PEEP > 5 cm H2O was an independent risk factor for oxygen desaturation. Receiving > 6 suctionings per day was a risk factor for desaturation and hemorrhagic secretions. The use of guidelines was independently associated with fewer complications.
CONCLUSIONS: Endotracheal suctioning frequently induces adverse effects. Technique, suctioning frequency, and higher PEEP are risk factors for complications. Their incidence can be reduced by the implementation of suctioning guidelines.
Introduction
The presence of an artificial airway during mechanical ventilation makes coughing less effective or not possible. Endotracheal suctioning is therefore needed to avoid accumulation of secretions into the lung, and its associated complications. Nevertheless, endotracheal suctioning is an invasive procedure, and is not free from hazards and, exceptionally, from lethal adverse events.1 Numerous side effects of endotracheal suctioning have been reported.2–11 Some old studies on selected patient populations suggested a high frequency of specific adverse events, such as oxygen desaturation and arrhythmia.1,12 Leur and co-workers13 reported a relatively low incidence of some endotracheal suctioning adverse events in a selected population of surgical patients without ARDS and with a short duration of mechanical ventilation. Thus, the incidence and risk factors of adverse effects of endotracheal suctioning in a general medical population of critically ill patients are uncertain.
In 2010 the American Association for Respiratory Care published updated clinical practice guidelines for endotracheal suctioning,9 with the aim of optimizing the procedure and reducing the hazards. Specific suctioning strategies are not systematically used in ICUs,14 and their usefulness has not been well assessed. Moreover, the optimal approach to reduce endotracheal-suctioning-related complications has not been fully clarified.15,16 Therefore we carried out a clinical investigation to evaluate the incidence of endotracheal-suctioning-associated adverse events in mechanically ventilated patients, and to determine whether the implementation of practice guidelines could decrease the rate. Suctioning-induced adverse events before and after the implementation of practice guidelines were compared using the same methodology. Practice guidelines for endotracheal suctioning were drafted independently from those of the American Association for Respiratory Care,9 and before their release.
QUICK LOOK
Current knowledge
Endotracheal suctioning is associated with various complications, ranging from discomfort to hemodynamic collapse, but the incidence and severity of these complications has not been systematically studied. The usefulness of adherence to suctioning guidelines has also not been addressed.
What this paper contributes to our knowledge
Adverse effects of suctioning, particularly oxygen desaturation and hemorrhagic secretions, were frequent and were reduced by the implementation of practice guidelines. Factors that increased the risk of suctioning-related complications included more frequent suctioning, requirement for a PEEP of > 5 cm H2O, and the presence of ARDS.
Methods
Study Location and Subject Population
The study was conducted in the 26-bed medical ICU of Henri Mondor University Hospital, Créteil, France. The institutional ethics committee approved the study and waived the requirement for informed consent. All consecutive patients needing mechanical ventilation and ≥ 18 years old were included during two 3-month periods, from February to April 2000 (period 1) and from April to June 2001 (period 2). According to clinical requirements, subjects received sedation by continuous infusion, following our local protocol, which was the same in the 2 study periods. They were mechanically ventilated with volume controlled continuous mandatory ventilation or pressure support mode. Heat and moisture exchangers were generally used. In all subjects, pulse oximetry, electrocardiography, and arterial blood pressure were continuously monitored, according to routine practice.
Study Design and Data Collection
Endotracheal-suctioning-related adverse events were collected daily during the 2 3-month periods. During the first period, endotracheal suctioning was performed according to the usual practice at that time: suctioning procedures were mainly performed routinely every 2 hours or more often if secretions were visible in the endotracheal/tracheostomy tube; subjects were disconnected from the ventilator; the duration of the procedure, the vacuum pressure (frequently > 400 cm H2O), size of the suction catheter, and depth of suctioning were not standardized; saline was instilled in case of dry, tenacious secretions; no special precaution was used in subjects with ARDS; in general, closed suction systems were not used.
In the 1-year interval between the 2 study periods, clinical practice guidelines for endotracheal suctioning were developed during the first month based on the available evidence, and subsequently implemented. The rationale and the feasibility of each guideline were discussed in depth with physicians and nurses until a consensus was reached and, finally, guidelines were described in a written protocol. To facilitate implementation, repeated meetings were organized to educate and to instruct the whole personnel about this protocol. Repeated informal follow-up training was also performed, and a medical referent was always available for any questions and technical needs.
In the second period, endotracheal suctioning was performed according to practice guidelines. No major change took place in the unit in between these 2 periods regarding airway and ventilator management. During the 2 study periods, nurses were instructed to detect and report daily on standardized data collection sheets all adverse events for each suctioning procedure. During and just after the intervention period (period 2), adherence to practice guidelines was also assessed by respiratory therapists and physicians not involved in suctioning procedures. They randomly observed suctioning procedures and, for each procedure, reported if guidelines were followed. A total of 600 observations were performed during night and day. Nurses were not informed of the observers' task.
Adherence to the study protocol was assessed daily by investigators and respiratory therapists. This was done by comparing the number of suctioning procedures reported on the subject's daily clinical chart and the number of procedures reported on the specific daily sheet used for the study. In addition, in an attempt to validate the reliability of detecting and reporting adverse effects of endotracheal suctioning following the given instructions, one of the investigators repeatedly observed suctioning procedures and reported if these instructions were followed. Reliability in reporting adverse events of suctioning was calculated as:
Number of correctly reported events/number of observations × 100
A total of 540 observations were performed: 270 in each period.
Clinical Practice Guidelines for Endotracheal Suctioning
The guidelines for endotracheal suctioning were as follows:
Frequency of Endotracheal Suctioning. The suctioning procedures had to be performed according to the subject's needs, and not routinely.17 The need for endotracheal suctioning was evaluated based on oscillations on the expiratory part of the flow-time curve18 and tracheal or bronchial respiratory sounds.19,20 Ventilator alarms (increased peak airway pressure during volume controlled continuous mandatory ventilation, or decreased tidal volume during pressure-targeted ventilation modes), presence of secretions in the endotracheal tube or oxygen desaturation, after excluding other possible causes, were also considered as later indicators of the need for suctioning. In paralyzed subjects, endotracheal suctioning was performed every 4 hours, even if the aforementioned signs were absent.
Disconnection from the ventilator had to be avoided. The suction catheter was introduced through the swivel adapter of the catheter mount, or a closed system was used.6
Depth of Endotracheal Suctioning. To minimize mucosal trauma, shallow suction (limited to the artificial airway and the trachea) was performed, instead of deep suctioning.13 In practice, approximately 8–10 cm of the suction catheter was left outside the endotracheal tube. With a tracheostomy the suction catheter was introduced up to approximately half its length. In any case, insertion was stopped if an obstacle was met, and the suction catheter was withdrawn approximately 1 cm. Suctioning was then started while gradually withdrawing the catheter.
Instillation of saline was avoided.21–23 In case of dry, tenacious secretions, the heat and moisture exchanger was replaced by a heated humidifier. Selective suctioning under direct visualization by fiberoptic bronchoscopy was performed if a mucus plug was suspected.
Size of the Suction Catheter. This had to be adapted to the size of the endotracheal tube, so that the diameter of the suction catheter was < 50% the inner diameter of the artificial airway.10,11,17,24,25 In practice, 16 French suction catheters were used with artificial airways with an inner diameter ≥ 9 mm, 14 French suction catheters were used with 8.0-mm or 8.5-mm endotracheal tubes, and 12 French catheters with 7.0-mm or 7.5-mm endotracheal tubes.
The duration of endotracheal suctioning was limited to < 10–15 seconds.17,26,27 If needed, the suctioning procedure was repeated after a time period sufficient for restoring baseline ventilation and oxygen saturation.
The suction pressure had to be set between 200 and 250 mm Hg.17,25,27,28
In subjects with ARDS, to minimize suctioning-induced lung derecruitment, a closed suction system was used, and ventilator auto-triggering was allowed during the procedure.5,6 Closed suctioning systems were changed in case of mechanical failure or visible soiling only: not routinely.23,29–31 Recruitment maneuvers were used in case of persisting hypoxemia after suctioning.4,32
A sterile technique was employed at all times. The subject's appearance (eg, sweating, skin color, agitation), vital signs (oxygen saturation, heart rate, cardiac rhythm, arterial blood pressure), and ventilatory parameters (breathing frequency, tidal volume, peak inspiratory pressure) were monitored during the whole suctioning procedure.17,27
Adverse Effects of Endotracheal Suctioning
Adverse effects of endotracheal suctioning were defined a priori, as follows:
Oxygen desaturation: an SpO2 decrease of > 5%
Hemorrhagic secretions: blood visible in suctioned secretions
Severe hypertension: an increase in systolic blood pressure to > 200 mm Hg
Severe hypotension: a drop in systolic blood pressure to < 80 mm Hg
Severe tachycardia: an increase in heart rate to > 150 beats/min
Severe bradycardia: a decrease in heart rate to < 50 beats/min
Arrhythmia: any new appearance of sustained supraventricular or ventricular arrhythmia
Statistical Analysis
Results are reported as mean ± SD, except when otherwise indicated. Incidence density, expressed per 100 ventilator days, was calculated according to the formula:

Dichotomous variables were compared with use of the chi-square test, and continuous variables with the Student t test. After assessing normality, the continuous variables were dichotomized using adequate cut-points. Logistic regression analysis was performed, incorporating all factors with P < .10 in the univariate analysis. A P ≤ .05 in a 2-tailed test was used to indicate significance. All analyses were performed using statistics software (StatView 5, SAS Institute, Cary, North Carolina).
Results
We included 147 subjects, and 9,500 suctioning procedures were recorded during a total of 1,225 ventilator days. During the pre-intervention 3-month period (period 1), 4,506 suctioning procedures in 79 subjects were collected during 604 ventilator days. After guidelines implementation (period 2), 4,994 suctioning procedures, in 68 subjects, were collected during 621 ventilator days.
Nurse reliability in detecting and reporting suctioning adverse effects was 94% overall, varying from 91% in period 1 to 96% in period 2. The most common errors in reporting adverse events concerned severe hypotension (20%) and oxygen desaturation (17%). The comparison between the number of suctioning procedures reported on the subject's daily chart and the number of procedures reported on the specific daily sheet used for the study showed that endotracheal suctioning procedures were adequately reported in 95.2% of cases, varying from 94.8% in period 1 to 95.6% in period 2. As shown in Table 1, the general characteristics of the subjects, number of collected suctioning procedures, and outcomes were not statistically different between the 2 periods.
Subjects, Outcomes, and Number of Suctioning Procedures
Adverse Effects of Endotracheal Suctioning Before Guidelines Implementation
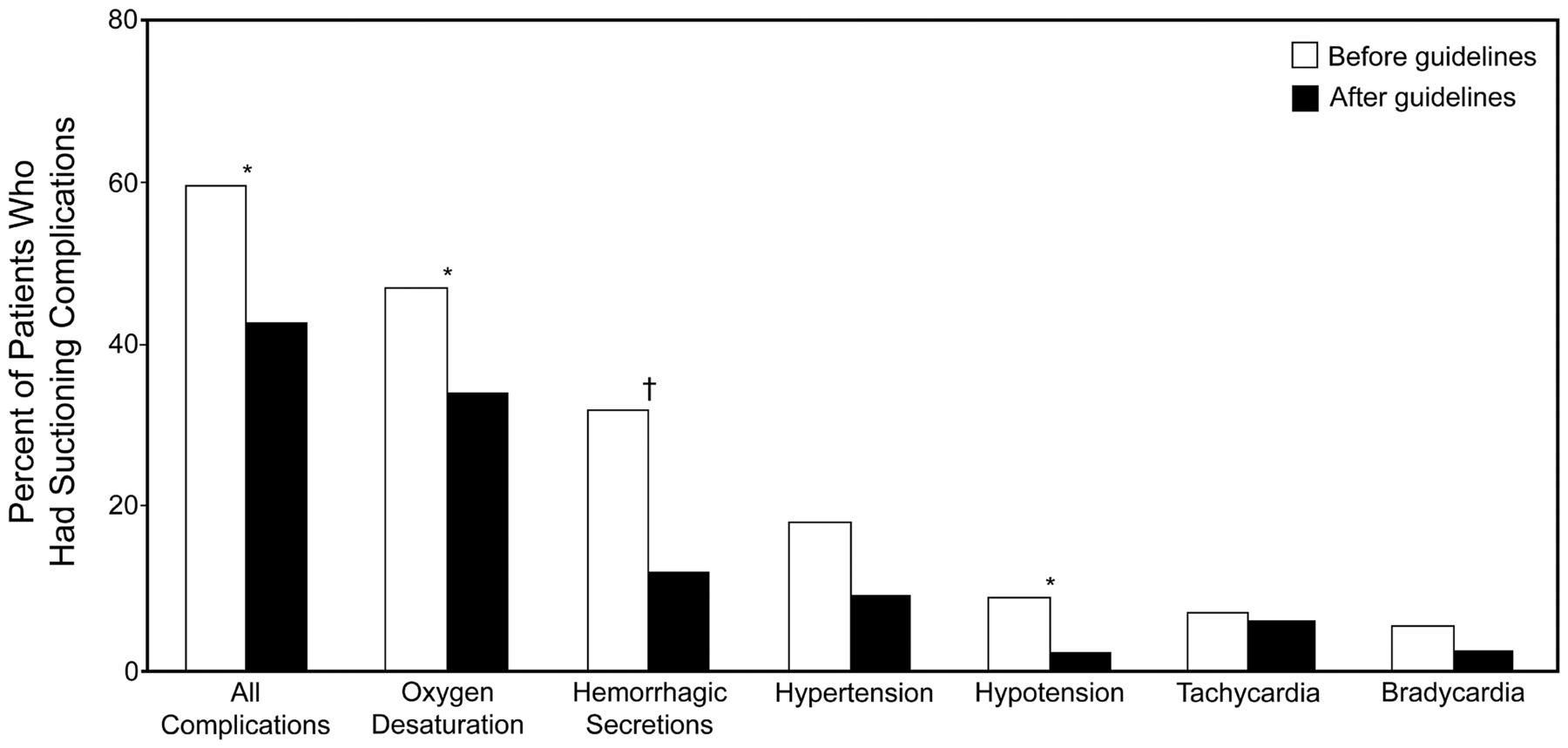
In period 1, 47 subjects (59.5%) experienced at least one complication from endotracheal suctioning: oxygen desaturation occurred in 37 subjects, hemorrhagic secretions in 25, hypertension in 14, hypotension in 7, tachycardia in 5, and bradycardia in 4 (Fig. 1). One subject experienced transient ventricular tachycardia, which resolved spontaneously after suctioning. Adverse effects occurred in 559 procedures (Fig. 2) and 173 ventilator days (Fig. 3), which calculated to a rate of endotracheal-suctioning-associated adverse effects of 92.5 per 100 ventilator days. Oxygen desaturation (incidence density of 48.3 per 100 ventilator days) and hemorrhagic secretions (incidence density of 30 per 100 ventilator days) were the most frequent adverse effects.
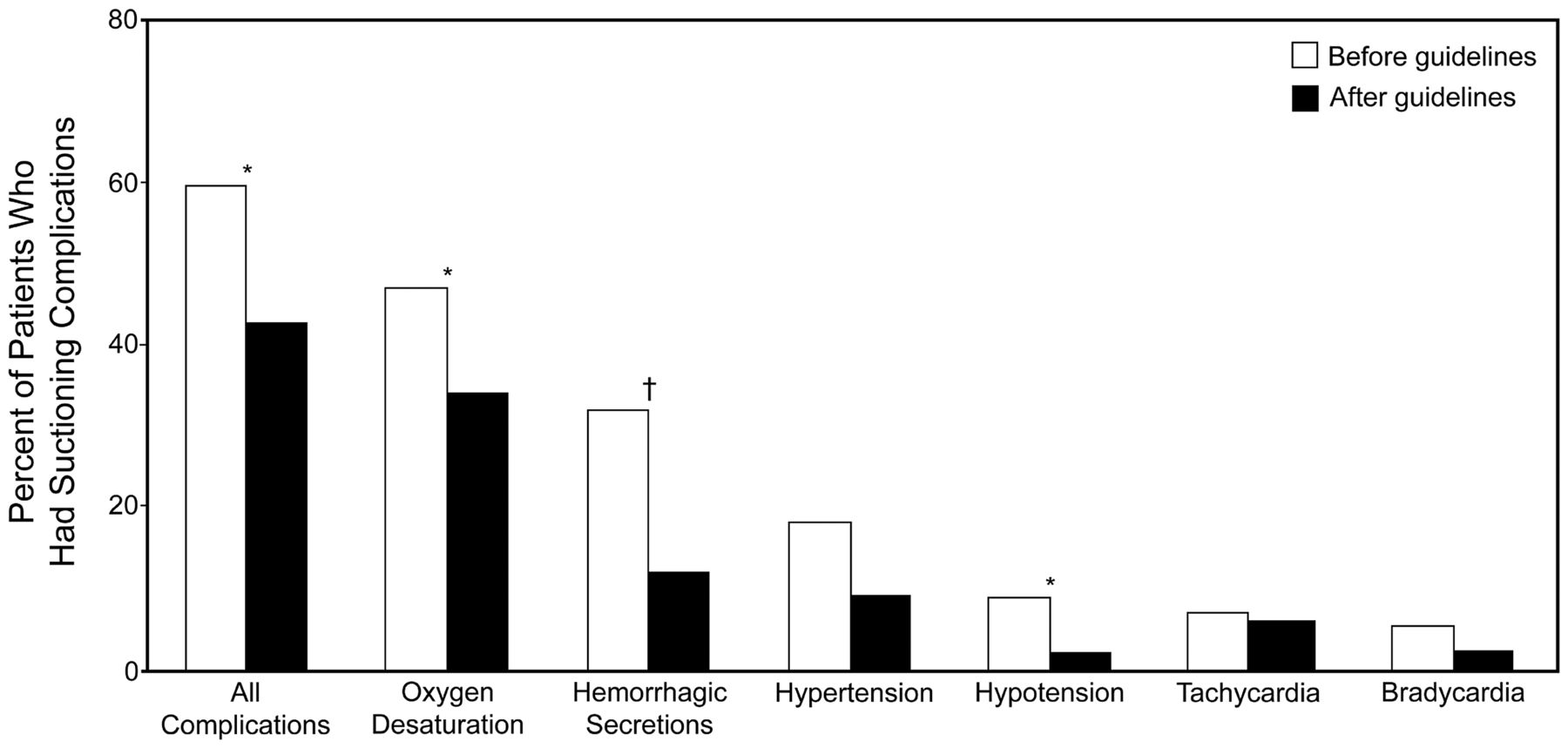
Mean percentages of subjects who suffered adverse effects from endotracheal suctioning. The sum of proportions for specific complications is greater than the percentage for all complications, because several complications could occur with a single procedure. * P < .05. † P = 004.
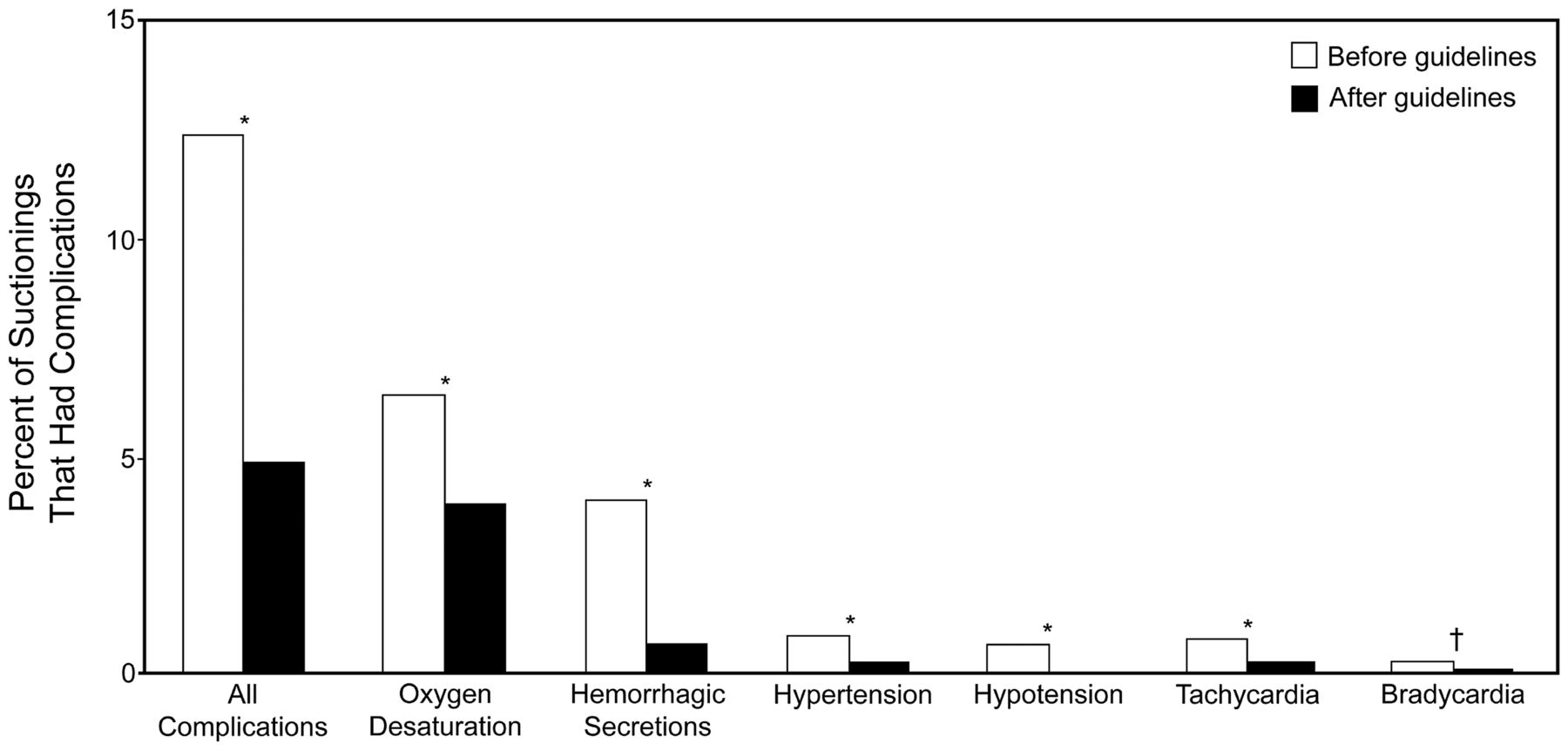
Mean percentages of suctioning procedures that had complications. The sum of proportions for specific complications is greater than the percentage for all complications, because several complications could occur during a single procedure. * P < .001. † P = .006

Mean percentages of ventilator days on which suctioning procedures had complications. The sum of proportions for specific complications is greater than the percentage for all complications, because several complications could occur during a single procedure. * P < .001. † P = .01 ‡ P = .05.
Effect of Practice Guidelines on Endotracheal-Suctioning-Associated Adverse Effects
Adherence to practice guidelines was 95.9%. The effects of guidelines implementation are shown in Figures 1, 2, and 3. Compared to period 1, the proportion of subjects experiencing any complication from endotracheal suctioning was significantly reduced after guidelines implementation (P = .04). Particularly, fewer subjects presented hemorrhagic secretions (P = .004), hypotension (P = .04), and, after adjusting for the duration of mechanical ventilation, oxygen desaturation (P = .02). No subject presented any form of arrhythmia during period 2. The rate of complicated suctioning procedures was reduced by 61% in period 2, with a rate of endotracheal-suctioning-associated adverse effects of 39 per 100 ventilator days (P < .001). This reduction concerned all adverse effects, with a decrease of 40% for oxygen desaturation (incidence density of 31.1 per 100 ventilator days) (P < .001), 83% for hemorrhagic secretions (5.5 per 100 ventilator days) (P < .001), 78% for hypertension (1.8 per 100 ventilator days) (P < .001), 94% for hypotension (0.3 per 100 ventilator days) (P < .001), 75% for tachycardia (1.8 per 100 ventilator days) (P < .001), and 67% for bradycardia (0.6 per 100 ventilator days) (P = .006). The proportion of days of mechanical ventilation with complicated suctioning procedures was also significantly reduced in period 2 (P < .001). Oxygen desaturation and hemorrhagic secretions remained the most frequent adverse effects. In period 2 the proportion of subjects with frequent suctioning procedures (> 6/d) was lower, albeit not significantly, than in period 1 (see Table 1).
Risk Factors for Endotracheal-Suctioning-Associated Adverse Effects
For the analysis, hypertension and hypotension were grouped together into a “blood pressure changes” category, and tachycardia and bradycardia were grouped into a “heart rate changes” category. The results of the univariate analysis for individual and grouped adverse effects are shown in Table 2. General characteristics were not different between subjects with or without endotracheal-suctioning-associated adverse effects. For all adverse events, frequency of suctioning was significantly higher in subjects with adverse effects than those without. Subjects exhibiting oxygen desaturation during endotracheal suctioning had a higher frequency of ARDS, were ventilated with a PEEP higher than 5 cm H2O, and had an FIO2 greater than 0.6 more frequently than subjects who did not present oxygen desaturation. Anticoagulation for at least 3 days was more frequent in subjects with hemorrhagic secretions than in those who did not present such complication.
Univariate Analysis of Complications of Endotracheal Suctioning
The results of the multivariate regression analysis are shown in Table 3. Only PEEP > 5 cm H2O and > 6/d suctioning procedures were independently associated with an increased risk of oxygen desaturation during suctioning. By contrast, not having ARDS and being in period 2 were independent protective factors for desaturation. Frequency of suctioning (> 6/d), but not anticoagulation, was independently associated with an increased risk of hemorrhagic secretions, while period 2 was a protective factor for this complication. The only independent risk factor for suctioning-induced blood pressure changes was the occurrence of oxygen desaturation.
Multivariate Logistic Regression Analysis
Discussion
The main results of this study are that:
Endotracheal suctioning was frequently complicated, mainly by oxygen desaturation and hemorrhagic secretions.
The implementation of practice guidelines reduced the incidence of all adverse effects.
Frequent suctioning, PEEP > 5 cm H2O, and ARDS were risk factors for the main adverse events (oxygen desaturation and hemorrhagic secretions).
Oxygen desaturation was a risk factor for hemodynamic alterations during endotracheal suctioning.
The first step of our education initiative to reduce adverse effects from endotracheal suctioning was to assess their incidence during current practice. In this study a large proportion of mechanically ventilated subjects experienced adverse events when endotracheal suctioning was not protocolized. Previous small clinical studies have reported several complications of endotracheal suctioning.1,3,5,6,12 In a population of mostly surgical patients with a relatively short duration of mechanical ventilation (4–5 d) and without ARDS, Leur et al found that complications of routine endotracheal suctioning occurred in 38.6% of procedures.13 When a less invasive suctioning technique was adopted (using a modified suction catheter), complications were reduced to 28.6%. In the first period of our study (routine suctioning), we found a smaller incidence of hypertension and arrhythmia, but a larger incidence of oxygen desaturation than previously reported.13 Differences in the definition of complications, in suctioning techniques, and in patient population likely explain these discrepancies. Instead of relative changes, we used absolute cutoff values for blood pressure and heart rate modifications, to facilitate the task of reporting adverse effects for nurses. As a consequence, we could have underestimated these complications. Not surprisingly, we found a greater incidence of oxygen desaturation than in Leur's study, in which patients with severe acute respiratory failure were excluded.13 Our subjects were sicker, and approximately 20% of them had ARDS (see Table 1). In particular, their illness severity was slightly greater, although not significantly, in period 2, as suggested by the slightly higher Simplified Acute Physiology Score II and greater incidence of ARDS. This can probably explain the somewhat longer duration of mechanical ventilation and ICU stay, and the trend toward lower ICU survival in period 2 (see Table 1).
Our data suggest the usefulness of practice guidelines to reduce the hazards of endotracheal suctioning.9,11,23 In particular, our results support the clinical value of the recently updated clinical practice guidelines of the American Association for Respiratory Care.9 Our guidelines, independently developed on the basis of available evidence, are in fact very similar, although there may be some differences, mainly related to the control of the depth of suctioning. Our method consisted of leaving approximately 8–10 cm of the suction catheter outside the endotracheal tube, or, in the extreme case of a too deep insertion of the suction catheter inside the trachea so that an obstacle was met, of withdrawing the suction catheter before applying the negative pressure. This method may be imprecise for determining suction depth, and it does not precisely reflect the recent clinical practice guidelines of the American Association for Respiratory Care.9 The use of suction catheters with length marks would be the best solution to perform shallow suctioning. Unfortunately, we did not have these catheters available in our ICU, as is still the case in many ICUs. Our protocol, including the technique of suctioning, was designed to make the individual tasks as easy as possible with the available means. Nevertheless, we observed a quite striking decrease in the rate of hemorrhagic secretions in period 2, suggesting that a lower rate of mucosal trauma should have occurred after the implementation of guidelines, and supporting the idea that the depth of suctioning was indeed reduced in period 2. The bleeding rate could have been even lower with a more precise control of the depth of suctioning. Our study design did not permit us to determine the weight of each recommendation on the global impact of guidelines implementation on adverse effects of endotracheal suctioning.
Endotracheal-suctioning-induced oxygen desaturation results from lung derecruitment secondary to both the loss of positive airway pressure due to ventilator disconnection and the application of negative pressure, particularly in patients with ARDS.3,5,6,11 The duration of the suctioning procedure, the level of the applied negative pressure, the size of the suction catheter, and instillation of saline may also influence the occurrence of lung derecruitment and hypoxia.10,11,25–27 Accordingly, the partial prevention of derecruitment obtained by avoiding ventilator disconnection or using a closed system in ARDS patients,5,6,11 while limiting the duration of procedure, the level of the negative suctioning pressure, and the size of the suction catheter, can explain the observed decrease in oxygen saturation after guidelines implementation. The presence of blood in suctioned secretions is likely explained by airway mucosal trauma caused by repeated introductions of the suction catheter and application of negative pressure. In agreement with a previous study,13 the reduced depth of suctioning and the limitation of negative pressure provided by our protocol can account for the large decrease in the rate of hemorrhagic secretions in period 2. A further limitation of the suction pressure might have been associated with a further reduction of oxygen desaturation and hemorrhagic secretions, but this might have also reduced the efficacy of suctioning in clearing secretions. Blood pressure and heart rate modifications can result from abrupt changes of intrathoracic pressure, the release of endogenous catecholamines secondary to suctioning-induced stress, hypoxemia, and vagal stimulation.1,13,33
To our knowledge this is the first study assessing risk factors for adverse effects of endotracheal suctioning. This may be useful in identifying patients at increased risk for suctioning-related complications. We found that subjects with ARDS, and subjects ventilated with high PEEP, were at an increased risk of oxygen desaturation (see Table 3). We have previously shown in ARDS subjects that lung derecruitment observed after ventilator disconnection was correlated with the level of applied PEEP.6 Here we could quantify the degree of hypoxemic risk conferred by PEEP > 5 cm H2O (a 196% increase in risk). In addition, we showed that frequent suctioning procedures (> 6/d) substantially increase the risk of oxygen desaturation and hemorrhagic secretions (see Table 3). No risk factor was found for heart rate changes, likely because of their low incidence, whereas oxygen desaturation was the only identified prognostic factor for arterial blood pressure alterations (see Table 3). This confirms previous data suggesting that hypoxemia plays a key role for the occurrence of this complication.33
The 2 suctioning procedures were applied sequentially, in 2 different periods, and not randomized. Although randomization might have allowed a more rigorous study design, the contemporaneous use of 2 different suctioning procedures would have been a source of confusion for the nursing staff, potentially leading to major protocol deviations. In addition, the study was designed as an education initiative, and the study protocol was designed to make the individual tasks as easy as possible. The high adherence obtained with this approach may have compensated at least in part for the less rigorous study design. We did not compare directly the efficacy of the 2 suctioning procedures, which would require a different study design. All our recommendations were based on the literature, however, and on our own experiments.6
Conclusions
The adverse effects of endotracheal suctioning, particularly oxygen desaturation and hemorrhagic secretions, are frequent and can be reduced by the implementation of practice guidelines. Several factors can be used to identify patients at higher risk of airway-suctioning-related complications so that we can pay more attention to high-risk patients and target future intervention studies toward those patients most likely to benefit.
Acknowledgments
We thank Graça Salgueiro and Véronique Morisset (nurses) and Sylvie Lely and Nicole Jackson (respiratory therapists) for their constant support, and Jérôme Pigeot and Solenne Taillé (biomedical engineers) for technical assistance.
Footnotes
- Correspondence: Salvatore Maurizio Maggiore MD PhD, Department of Anesthesiology and Intensive Care, Agostino Gemelli Hospital, Catholic University of the Sacred Heart, Largo Agostino Gemelli 8, 00168 Rome, Italy. E-mail: smmaggiore{at}rm.unicatt.it.
Dr Maggiore presented a version of this paper at the International Conference of the American Thoracic Society, held May 17–22, 2002, in Atlanta, Georgia.
The authors have disclosed no conflicts of interest.
See the Related Editorial on Page 1707
- Copyright © 2013 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}