

Abstract
Despite the accepted importance of minimizing time on mechanical ventilation, only limited guidance on weaning and extubation is available from the pediatric literature. A significant proportion of patients being evaluated for weaning are actually ready for extubation, suggesting that weaning is often not considered early enough in the course of ventilation. Indications for extubation are often not clear, although a trial of spontaneous breathing on CPAP without pressure support seems an appropriate prerequisite in many cases. Several indexes have been developed to predict weaning and extubation success, but the available literature suggests they offer little or no improvement over clinical judgment. New techniques for assessing readiness for weaning and predicting extubation success are being developed but are far from general acceptance in pediatric practice. While there have been some excellent physiologic, observational, and even randomized controlled trials on aspects of pediatric ventilator liberation, robust research data are lacking. Given the lack of data in many areas, a determined approach that combines systematic review with consensus opinion of international experts could generate high-quality recommendations and terminology definitions to guide clinical practice and highlight important areas for future research in weaning, extubation readiness, and liberation from mechanical ventilation following pediatric respiratory failure.
- weaning
- extubation
- mechanical ventilation
- respiratory support
- spontaneous breathing
- stridor
- pressure rate product
- esophageal pressure measurements
- respiratory inductance plethysmography
- phase angles
- maximum negative airway pressure
Introduction
An extensive review paper on weaning and extubation readiness in pediatric patients from the Collaborative Pediatric Critical Care Research Network published in 20091 pointed out that there were many myths, unique practices, little consensus, and less objectivity surrounding this important pediatric critical care activity. Recently, Rimensberger et al2 placed lack of guidance regarding weaning and extubation as being one of the top 10 unknowns in pediatric mechanical ventilation. It is the intent of this review to summarize progress that has been made in weaning and extubation readiness assessments since the 2009 review and to address the benefits of some newer physiological methods and technology applications in this field of investigation.
The course of conventional mechanical ventilation begins with intubation and the provision of ventilatory support. As the acute phase of the disease subsides, weaning begins. The end of weaning can be defined as the time at which the patient’s spontaneous breathing alone provides effective gas exchange and clinical stability, although how this point can best be determined is unclear. At the end of weaning is extubation, or the act of liberation from the ventilator and endotracheal tube (ETT).
Background
The length of weaning depends on a number of factors, among them fluid status. When total body water increases, lung compliance decreases due to increased lung water, chest wall, and diaphragm edema. In adults with ARDS, it is clear that the injured lungs should be managed dry.3,4 Patients managed with a conservative fluid regime had fewer mechanical ventilation days and a quicker return of normal lung function than those receiving a more liberal regime.3 The importance of fluid balance in children is not as clear, although observational data in pediatric ARDS are also supportive.5-7 Respiratory losses in children are about one third of the total daily fluid intake. Because inspired gases in mechanical ventilation are humidified, it is probably prudent to limit total fluid intake (after initial resuscitation) to two thirds of normal.
PEEP management is another factor that may affect the length of weaning. While initiation and escalation of PEEP generally improves oxygenation in patients with ARDS, practitioners infrequently change PEEP levels, even after oxygenation improves.8,9 There may be a number of reasons for this. In part, this can be due to a concern about the effects of increased PEEP on cardiac output and pulmonary vascular resistance, which have been shown of little consequence in pediatric ARDS where the lungs are stiff and transmit less airway pressure.10-12 This reluctance to increase PEEP as recommended by the Pediatric Acute Lung Injury Consensus Conference13 may have long-term consequences of increased mortality.14 The slow weaning of PEEP may also obscure earlier recognition of the patient actually being ready for extubation. It is generally recommended that PEEP levels should be physiologic at the time of extubation (ie, ≤ 5 cm H2O),15 although extubation from higher PEEP levels may be important to maintain lung recruitment for certain types of patients (eg, obesity, obstructed airways).16,17 Sedation further complicates weaning and extubation.18,19 Oversedation may depress central respiratory drive, whereas undersedation can leave a child restless. Thrashing movements can result in airway trauma from the ETT.20,21 Two groups have shown an association between sedation level and extubation readiness, but this has not been validated prospectively in infants and children.19,22 Sedation assessment tools have been developed for this purpose and may be helpful in targeting a particular level of sedation;18,23 however, implementation of a nurse-driven protocol to achieve these targets did not appear to have a significant impact on weaning times.20
Pulmonary hypertension is another important factor in determining readiness for weaning because of its effect on the patient’s oxygenation.24,25 Supplemental oxygen, continuous inhalation of nitric oxide through the ETT, and ventilatory support are the mainstays of treatment for pulmonary hypertension, and there is reluctance to withdraw these too quickly in the absence of direct measures of pulmonary arterial pressure or resistance.
Differences in diaphragmatic function may relate to longer weaning times in infants and young children. Accessory respiratory muscles are not as developed as in older children.26 As diaphragmatic dysfunction develops with prolonged mechanical ventilation, the duration of weaning can increase.27-30
As it does in another cause of subglottic edema in children (ie, croup), intermittent or continuous inhalations of epinephrine may prevent extubation failure by reducing subglottic mucosal edema.31 Steroids may also play a role in preventing re-intubation by reducing tracheal inflammation and subglottic edema associated with tracheal injuries from the ETT.32 One randomized controlled trial in children reported that steroids prevented upper-airway obstruction.33 Another randomized controlled trial also showed benefit, but given the high incidence of hypoalbuminemic edema in the study population the results may not be generalizable.34 The only other such study did not show benefit.35 Studies in adults indicate that steroids may be helpful for high-risk patients, defined on the basis of low cuff leak volume.36 A Cochrane Review37 on the role of steroids concluded that:
Using corticosteroids to prevent (or treat) stridor after extubation has not proven effective for neonates or children. However, given the consistent trend toward benefit, this intervention does merit further study. In adults, multiple doses of corticosteroids begun 12–24 h prior to extubation do appear beneficial for patients with a high likelihood of postextubation failure.
Finally, other factors are probably important to the weaning process, but there is a dearth of research in these areas, and they are not further discussed. These include disease reversibility (rapid [respiratory syncytial virus bronchiolitis] vs slow [respiratory syncytial virus pneumonia/ARDS]), cardiac function, and postoperative, neurologic, and nutritional status.38
Predictive Indexes for Weaning
Several indexes have been developed to predict success in weaning and extubation. Although these indexes have been variably used in research, they have not found common use in clinical care, some because of their complexity and others due to a lack of proven benefit over clinical judgment in pediatric practice. Two of the more commonly cited indexes are described here.
The first index is the rapid shallow breathing index (RSBI), calculated as breathing frequency (f) divided by tidal volume (VT), or f/VT. The RSBI was devised by Yang and Tobin39 and is a good discriminator of weaning success and failure in adults. This test has become more widely used in adult practice and research with varying success. Recently, the issue has been revisited in a meta-analysis of 41 RSBI studies.40 An editorial by Connors41 that accompanied the meta-analysis suggested that, during weaning, the f/VT index can be thought of as a screening test with high sensitivity and low specificity, and therefore it should be used early in the course of mechanical ventilation to identify patients who can breathe on their own. Some investigators have demonstrated that RSBI normalized to body weight has some predictive ability in pediatrics,22,42 although these values are often very low by the time extubation readiness testing occurs, reinforcing the concept that these should be used early in the course of weaning.15 Specificity can perhaps be improved by applying a confirmatory test such as esophageal pressure trend measurements, which can be applied in a pediatric ICU setting.43-46 The second index is the compliance, resistance, oxygenation, pressure (CROP) index, which is calculated as (dynamic compliance × maximum negative inspiratory pressure × alveolar-arterial oxygen difference)/breathing frequency.
In pediatrics, Thiagarajan et al42 reported that spontaneous f < 45 breaths/min, spontaneous VT > 5.5 mL/kg, RSBI < 8 breaths/min/mL/kg body weight, and CROP index > 0.15 mL/kg body weight/breaths/min were good predictors of successful extubation. Baumeister et al22 used modified RSBI and CROP indexes to predict successful extubation. Their threshold values (RSBI < 11, CROP index > 0.1 mL/kg body weight/breaths/min) differed from those of Thiagarajan and coworkers.42
As with adults, conflicting studies by others have reported that these indexes did not reliably predict extubation outcome in children.22,47,48 Manczur et al48 studied 47 subjects on CPAP, 7 of whom failed extubation (14.9%), with low-tidal volume (< 6 mL/kg) and minute ventilation (< 180 mL/kg) associated with failure. RSBI did not predict outcome. We have recently reported that RSBI at the time of extubation does not reliably predict re-intubation (area under the curve median (IQR) 0.534 [0.443–0.624]), although it is associated with the duration of use of noninvasive ventilation after extubation.15
The RSBI has become moderately popular in adult ICUs and is a built-in function on several modern ventilators in its “adult” formula. Nonetheless, because there is a wide range of age groups with different f values, it may not be a good predictor of extubation success or failure in the pediatric population.42,49 Whether age-specific f/VT ratios could be better is currently unknown.
Volumetric Capnography
Hubble et al50 used volumetric capnography to predict successful extubation in 45 children. A volumetric capnogram plots CO2 concentration in airway gas against expired volume. The slope of an expired, single-breath CO2 waveform can be used to calculate the physiologic dead space (VD/VT). The investigators reported that VD/VT < 0.50 reliably predicted extubation success with 75% sensitivity and 92% specificity, whereas VD/VT > 0.65 identified subjects at risk for failure. Some investigators have been able to reproduce this, but others have noted that VD/VT has a very weak association with extubation failure.51,52 Volumetric capnography requires an arterial or a capillary blood gas, and the predictive ability may depend on the types of patients studied, degree of parenchymal lung disease, and VT generated.53
Techniques of Weaning
The most common approach to weaning infants and children is gradual reduction of ventilatory support. Weaning with intermittent mandatory ventilation or synchronized intermittent mandatory ventilation occurs by reducing the ventilator rate. With pressure support ventilation, the inspiratory pressure is initially set to provide the required support, and then it is reduced gradually. Pressure support is often combined with intermittent mandatory ventilation (synchronized or not) during weaning. Volume support and volume-assured pressure support are special forms of pressure support available in certain ventilators that guarantee a minimum VT per assisted breath. Weaning with volume support is semiautomatic, where the pressure support level required to maintain a certain VT is reduced automatically as respiratory mechanics improve. Extubation then occurs from a low level of ventilator support (more commonly in infants and children than in adults54) or after an extubation readiness test, which may be defined as a bundle of items that are used to assess the patient’s ability to be liberated from mechanical ventilation. In addition to maintaining adequate minute volume and gas exchange without excessive respiratory effort, this includes factors such as sedation level, fluid balance, adequacy of protective airway reflexes (eg, cough, gag, swallowing oral secretions), respiratory muscle strength assessment, and hemodynamic status.
A second school of thought recommends moderate amounts of ventilator support to rest the patient’s respiratory muscles and to perform a daily extubation readiness test. Mechanical ventilation is discontinued if the extubation readiness test is passed.55,56 This approach has been more commonly used to wean adult patients than children, although the importance of some sustained patient effort of breathing throughout the weaning phase is increasingly being recognized as a means to prevent ventilator-induced diaphragm dysfunction.29 To that extent, ventilator-induced diaphragm dysfunction is an increasingly recognized complication of mechanical ventilation, which may be exacerbated by certain weaning or ventilator-management strategies. Ventilator-induced diaphragm dysfunction further complicates weaning and therefore is an active area of investigation in both adult and pediatric critical care.57,58
In some patients, weaning is attempted with alternating periods of complete ventilatory support and graded spontaneous breathing with assistance. This “sprinting” is performed on the basis of the theory that the respiratory muscles can be slowly trained to sustain completely spontaneous breathing. There is currently little evidence that such an approach is an effective way of training muscles. There are also no data comparing such an approach with more traditional approaches of weaning.59 A multicenter randomized controlled trial comparing 3 modes of weaning reported no significant differences between having no protocol, weaning with pressure support, or weaning with volume support.19
It is important to recognize that not all patients require gradual weaning. Both adult and pediatric studies have reported that when patients pass a spontaneous breathing test and are subjected to an extubation readiness test, 50–75% of the patients are deemed ready to extubate and will do so successfully.19,49,55 Nonetheless, adult trials have often used standardized weaning protocols to minimize the time on a ventilator and provide uniform decisions about weaning.20,54,60-62 Studies in children have begun to follow suit, and the requirements for and utility of ventilator protocols in this age group have been reviewed.63-68 These weaning trials embraced a daily extubation readiness test, and all have used ventilator-free days as their primary outcome. The concept of ventilator-free days is implicitly based on having a low failed extubation rate from any cause other than the original cause of respiratory failure.69 This standard is being adopted in pediatric trials but may be inappropriate because not only is there a higher rate of failed extubations in this group, but up to 40% may involve upper-airway obstruction.21,63,70,71 Thus, for pediatric research, it may be important to define the end of successful weaning in a manner short of extubation. Whether the extubation is successful or unsuccessful may be of secondary importance for the purpose of a trial. This approach was taken by Schultz et al72 in their pediatric weaning study and was allowed in the ARDSNet low VT trial in adults,56 with both studies allowing achievement of minimum support settings short of extubation. Ideally, the timing of extubation should coincide with the determination that the patient is ready to sustain adequate gas exchange by spontaneous breathing alone. It is clear from the published studies that there is no such pediatric standard.
The use of a weaning protocol results in faster weaning in adults. Although the data are less clear in children, it is likely that a consistent approach to ventilator weaning will shorten ventilation times and result in better outcomes.66,68,72
Criteria for Readiness for Extubation
Readiness for extubation implies that weaning is completed, the patient is sufficiently awake with intact airway reflexes, is hemodynamically stable, and has manageable secretions. Extubation failure has been variably defined as re-intubation within 24–72 h. Tests commonly used to assess extubation readiness include testing for a leak around the ETT (ie, the leak test) and assessing respiratory muscle strength by measuring negative inspiratory force.
Leak Test
Upper-airway obstruction has been stated as a cause of up to 40% of failed extubations in children.21,71 Cuffed ETTs have been cited as a cause of increased upper-airway obstruction on extubation, but a variety of studies have reported no difference in the incidence of failed extubations over all age groups between those intubated with appropriately sized cuffed or uncuffed tubes.21,73-75
The leak test, whereby air is heard, without using a stethoscope, as a leak around the ETT at low pressure (usually < 20–25 cm H2O), is commonly used to predict upper-airway obstruction after extubation. However, it is not a very sensitive nor specific test.76-78 Wratney and coworkers79 analyzed the change in airway leak as measured at the time of intubation and extubation as a predictor of extubation outcome. They found that measuring the leak serially over time was a better predictor of extubation success than of extubation failure, although the clinical utility is unclear because the positive and negative likelihood ratios were near 1.
There appear to be important differences in the utility of leak measurements based on whether the ETT is cuffed or uncuffed. Some have attempted to make the leak test more objective.80 Cuff leak volume and leak percentage are calculated using standard ventilator settings (pressure control, heart rate = 10–20 beats/min, peak inspiratory pressure = 20 cm H2O; PEEP = 5 cm H2O). For uncuffed ETTs, leak percentage is calculated as (inspiratory VT minus expiratory VT)/(inspiratory VT). For cuffed ETTs, cuff leak volume is calculated as (expiratory VT with cuff inflated minus expiratory VT with cuff deflated)/(expiratory VT with cuff inflated). In a study of 409 infants and children immediately prior to their extubation, Khemani and colleagues21 reported that a cuff leak volume < 10% or a leak pressure (with the cuff deflated) > 25 cm H2O were highly associated with risk of upper-airway obstruction following extubation. The presence or absence of a leak was not associated with upper-airway obstruction for uncuffed ETT.
Negative Inspiratory Force
In the pediatric ICU, the negative inspiratory force test is usually performed quickly at the bedside with an uncalibrated manometer and with both inspiration and exhalation obstructed. The test has not been hitherto standardized nor validated in children as a test of extubation readiness, and hence it is unreliable under these conditions. One can reasonably conclude, nonetheless, that it is probably reassuring if a spontaneously breathing patient has a routinely obtained negative inspiratory force of ≥ 30 cm H2O. Similarly, consistently low values (ie, < 15 cm H2O), regardless of technique, are unlikely to be associated with successful weaning to extubation.
In a secondary analysis of the 409 children studied before and after extubation, Khemani et al15 noted that if a negative inspiratory force was performed in a standardized manner over 3–5 breaths, subjects with a maximum negative airway pressure of ≤ 30 cm H2O were nearly 3 times more likely to be re-intubated than if their maximum negative airway pressure was > 30 cm H2O (ie, reflecting good respiratory muscle strength).
Impact of ETTs on Weaning and Spontaneous Breathing Trials
Many clinicians believe that, for an infant or young child, respiring through a small ETT is akin to breathing through a straw, thereby imposing an unacceptable work of breathing. This notion is contrary to both clinical observation and physiology.45,81,82 Despite the fact that children were successfully extubated from CPAP prior to the advent of pressure support, it is often the practice to extubate children from levels of 5–10 cm H2O pressure support above PEEP to overcome the presumed increased effort of breathing. In a prospective trial, Khemani and coworkers46 used esophageal manometry to determine the pressure rate product on pressure support/PEEP and CPAP prior to extubation, and at 5 and 60 min afterwards. The pressure rate product is the breathing frequency times the peak-to-trough esophageal pressure and is a validated surrogate for work (or more correctly, effort) of breathing. In > 400 subjects, the authors were able to demonstrate that no matter how small the ETT (down to an inner diameter of 3.0 mm), effort of breathing on CPAP of 5 cm H2O best estimated postextubation effort. Furthermore, the pressure rate product on pressure support/PEEP was almost half of the level after extubation, therefore significantly underestimating the postextubation effort of breathing.83 The reasonable conclusion from this study is that, all things being equal, if a patient cannot breath comfortably on CPAP alone, then there is little chance he or she will do so when extubated (Fig. 1).46

Pressure rate product as a function of pre-extubation support (pressure support 10/PEEP 5 cm H2O), CPAP 5 cm H2O, and spontaneous breathing at 5 and 60 min postextubation. Data exclude 107 patients with postextubation upper-airway obstruction, stratified by ETT size. The patterns were the same for ETT size grouping of (A) ≤ 3.5 mm ID, n = 152; (B) 4.0–4.5 mm ID, n = 102; and (C) ≥ 5.0 mm ID, n = 48. Regardless of ETT subgrouping, pressure rate product on pressure support was less than CPAP (log transformed PRP, ANOVA, P < .0001). CPAP pressure rate product was similar to postextubation values (P > .05). ETT = endotracheal tube; ID = inner diameter. From Reference 46, with permission.
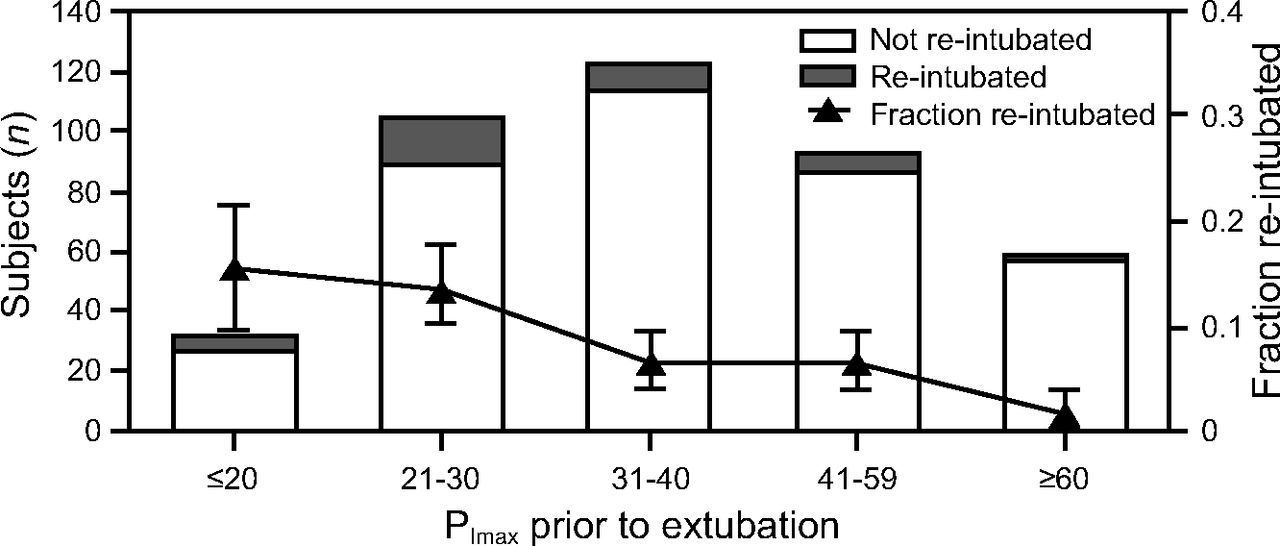
A further benefit of the pressure rate product is that, when evaluated along with maximum negative airway pressure, the combination of the former being > 500 and the latter being ≤ 30 cm H2O predicts high re-intubation rates of > 20%.15 These values reflect diminished respiratory muscle strength (ie, maximum negative airway pressure) in the face of high effort of breathing (ie, pressure rate product) (Fig. 2).
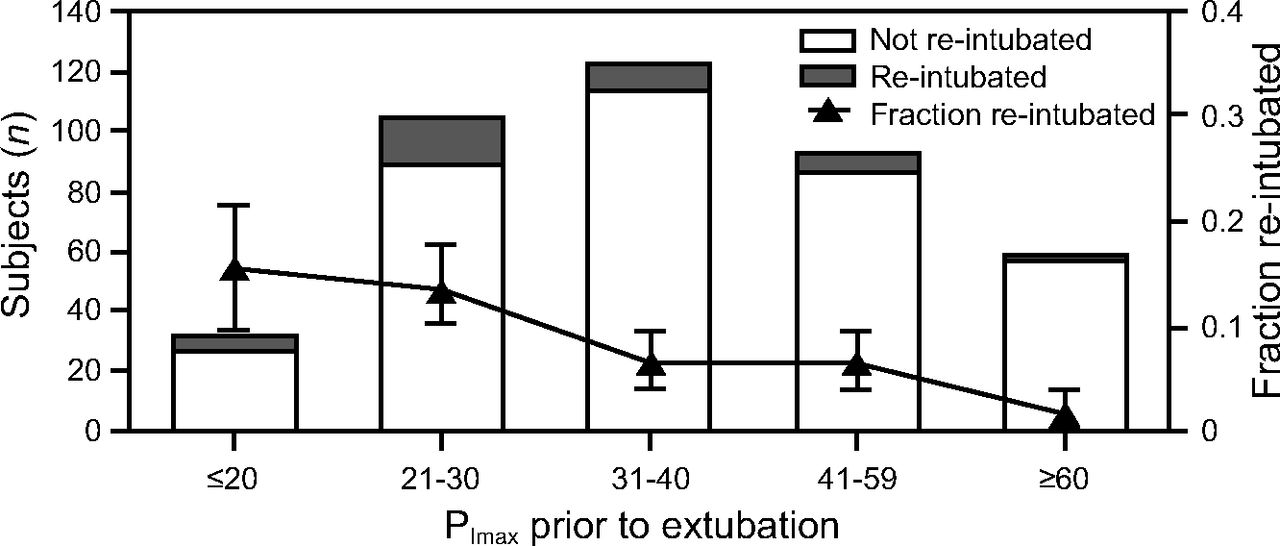
Maximum airway pressure during occlusion versus re-intubation. There is a dose-response relationship between lower maximum airway pressure during occlusion and re-intubation (test of trend, P = .01). Those with maximum airway pressure during occlusion of ≤ 30 cm H2O were a median of 2.8 (interquartile range 1.37–5.69) times more likely to be reintubated than those with a maximum airway pressure during occlusion > 30 cm H2O. From Reference 15, with permission.
Additional Technology for Assessment of Post-Extubation Upper Airway Obstruction
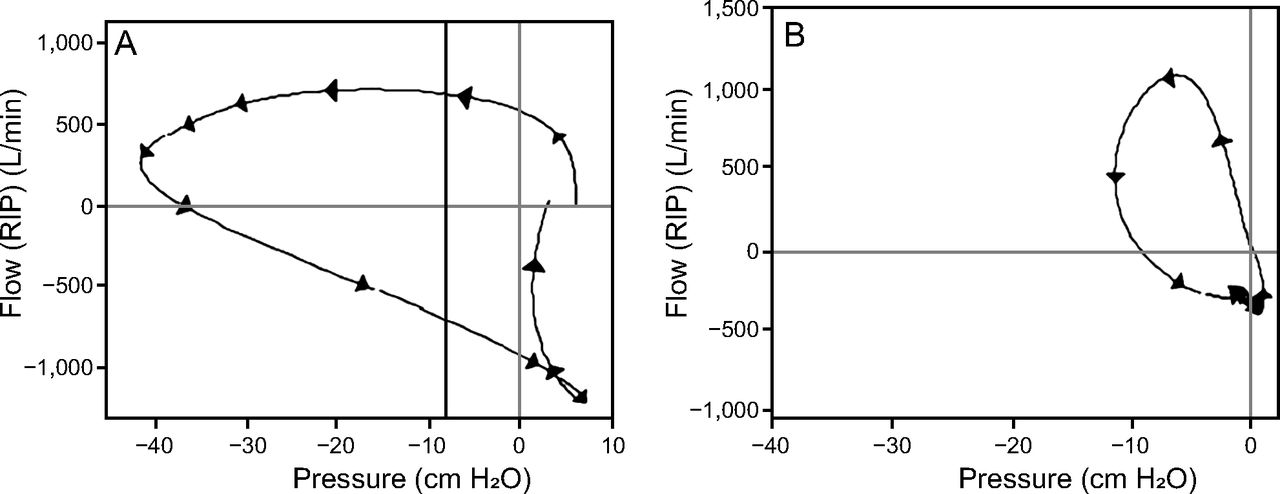
Upper-airway obstruction is common in a variety of pediatric diseases and is frequent after endotracheal extubation.21,84 Definitive data on risk factors and prevention of pediatric postextubation upper-airway obstruction are lacking. More objective measures of postextubation upper-airway obstruction severity in infants and children may help identify risk factors and elucidate optimal treatment or prevention strategies. Inspiratory flow limitation is relatively specific to extrathoracic upper-airway obstruction, characterized by disproportionately large inspiratory effort relative to flow. The most widely accepted method to measure flow is spirometry, which for non-cooperative spontaneously breathing children requires a tight-fitting mask over the nose and mouth, which may require sedation and may change flow dynamics.44 Respiratory inductance plethysmography is a less invasive alternative to spirometry.85 With respiratory inductance plethysmography, variations in the self-inductance of a coil (wires around the rib cage and abdomen) are measured as a result of changes in the cross-sectional area of the rib cage and abdomen. The combination of calibrated respiratory inductance plethysmography and esophageal manometry has shown promise for providing both an objective measure of the severity of postextubation upper-airway obstruction and some insights into risk factors for upper-airway obstruction. With the addition of a pneumotachograph on the ETT prior to extubation, respiratory inductance plethysmography flow can be calibrated during 3–5 breaths of airway occlusion during a negative inspiratory force procedure. This allows the construction of noninvasive flow-pressure loops from the respiratory inductance plethysmography and esophageal pressure measurements (Fig. 3).

A: Flow-pressure loops using spirometry. The flows are measured with a pneumotachograph (PNT) on the endotracheal tube. The pressure is obtained using an esophageal balloon catheter. B: Flow-pressure loops using respiratory inductance plethysmography (RIP). The flows are obtained from calibrated RIP belts around the thorax and abdomen at the same time as the recordings in (A), and the pressure is obtained using the same esophageal balloon catheter. From Reference 86, with permission.
These loops can be inspected for inspiratory flow limitation after extubation to characterize postextubation upper-airway obstruction. Patients can be observed as having upper-airway obstruction when inspiratory flow limitation is newly observed after extubation with an increase in pressure rate product of ≥ 50% over values before extubation while on CPAP (Fig. 4).

A: Flow-pressure loops using respiratory inductance plethysmography (RIP) for flow and esophageal manometry while intubated and breathing on CPAP. The loops are narrow and show no evidence of inspiratory flow limitation. B: Inspiratory flow limitation after extubation as subglottic narrowing occurs, as denoted by the flattened flow-pressure limb above the x axis. The pressure rate product has also increased 10-fold. From Reference 86, with permission.
The reversal of inspiratory flow limitation can also be seen after the child receives an upper-airway obstruction–specific intervention, such as inhaled racemic epinephrine (Fig. 5), heliox, or corticosteroids. Upper-airway obstruction can be further classified as subglottic if a jaw-thrust maneuver does not reduce the pressure rate product by ≥ 50%.21

A: Inspiratory flow limitation as denoted by the flattened flow-pressure limb above the x axis, and large negative change in esophageal pressure. B: The loops have narrowed after racemic epinephrine inhalation and show no evidence of inspiratory flow limitation. This is consistent with subglottic edema lessening after epinephrine administration. From Reference 21, with permission.
Summary
While we have made substantial improvements in our understanding of the unique and complex pathophysiology of weaning from mechanical ventilation through better clinical assessment and improved technological capabilities, there are still many unanswered questions and no clinical practice guidelines for ventilator liberation in children. An international initiative is currently underway to establish the first-ever pediatric ventilator liberation clinical practice guidelines (NIH/NICHD 1R13HD102137-01) and to prioritize areas of future research. Through continued investigation we will, hopefully, be able to accelerate the weaning process safely for many patients and to predict more accurately the likelihood of extubation success and avoid the complications and extended pediatric ICU stays that accompany failed extubations.
Footnotes
- Correspondence: Christopher JL Newth MD FRCPC FRACP, Division of Critical Care Medicine, Department of Anesthesiology & Critical Care Medicine, Children’s Hospital Los Angeles, MS #12, 4650 Sunset Blvd, Los Angeles, CA 90027. E-mail: cnewth{at}chla.usc.edu
Dr Newth presented a version of this paper at the New Horizons Symposium: Pediatric Respiratory Support of the AARC Congress 2019, held November 9–12, 2019, in New Orleans, Louisiana.
The authors have disclosed no conflicts of interest.
- Copyright © 2020 by Daedalus Enterprises
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.
- 62.↵
- 63.↵
- 64.
- 65.
- 66.↵
- 67.
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.
- 75.↵
- 76.↵
- 77.
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}