

Abstract
Although noninvasive ventilation (NIV) is administered to manage respiratory failure due to various causes, safety and effectiveness issues associated with the use of NIV masks have been reported. The present article aims to provide health professionals with a comprehensive review of the ergonomic considerations of NIV masks in terms of design, evaluation, and personalization. Based on a review of 93 papers, we provide guidelines for mask selection and troubleshooting during mask use as well as ergonomic approaches including face anthropometry, sizing systems, mask design, evaluation, and personalization. The comprehensive information presented in this review provides ergonomic perspectives to identify and prevent safety and usability problems associated with the use of NIV masks. Ergonomic improvement and personalization are important goals in order to facilitate the success of NIV treatment.
- noninvasive ventilation
- masks
- ergonomics
- safety
- user-centered design
- anthropometry
- computer-aided design
- printing
- three-dimensional
Introduction
Although noninvasive ventilation (NIV) is administered to patients with breathing difficulties to manage hypoventilation and respiratory failure, there are safety and effectiveness problems reported in association with NIV masks.1-2 The success of NIV treatment reduces the need for invasive ventilation, which increases the risk of infection and complications such as dysphagia, vocal cord palsy, and tracheomalacia.3 Various types of interface, including mouthpiece, oral (lip-seal mouthpiece) mask, nasal pillows, nasal mask, oronasal mask, total face mask, and helmet (Figure 1), are available for NIV treatment. However, excessive contact pressure caused by wearing a poorly fitting face mask can lead to discomfort, rashes, and pressure injuries.4-5 Although a small amount of air leakage from an NIV mask can lead to oronasal dryness, conjunctivitis, and sleep disturbance, a significant amount of air leakage can disturb NIV treatment due to patient-ventilator asynchrony.4-7 Problems with excessive pressure and air leakage due to a poorly fitting face mask cause 5–60% of cases of NIV failure.5

Types of noninvasive ventilation interfaces. A: Mouthpiece, B: oral (lip-seal mouthpiece) mask, C: nasal pillows, D: nasal mask, E: oronasal mask, F: total face mask, and G: helmet.
Ergonomic studies have been conducted to develop better mask designs in terms of safety, ease of use, and performance. Ergonomics is a discipline that applies the scientific knowledge of human beings to the development of designs that better fit the needs, capabilities, and limitations of users for safety, usability, comfort, and productivity.8-9 In this review, various mask types including oxygen masks (eg, NIV and pilot oxygen masks) and respirators (eg, dust mask with or without a filter) were examined. Although masks may be used in different use conditions,10-23 their ergonomic features and design requirements to achieve optimal fit to users can be similar. Mask designs based on the analyses of face shapes and sizes, mask sizing systems, representative faces, and/or digital headforms have been explored for better comfort and fit of a mask to the face.15,17,24-28 For example, Lee et al28 developed an ergonomically designed oxygen mask based on an analysis of face shapes and sizes, resulting in a 33–56% decrease in discomfort and a 11–33% decrease in contact pressure compared with existing masks. In addition, mask evaluations based on the analyses of subjective comfort, contact pressure, skin temperature, skin moisture, skin color, and/or air leakage have been conducted with physical and/or virtual mask prototypes to develop better mask designs.29-32 For example, as part of the evaluation of NIV mask designs, Riquelme et al33 measured the contact pressure at the physical interface between a mask and the face, whereas Lei et al34 estimated the contact pressure at the virtual interface between a mask model and a digital face using the finite element method. Finally, methods of designing a personalized mask, including 3-dimensional (3D) scanning of the face, modeling of a mask using computer-aided design (CAD) software, and fabrication of a personalized mask using a rapid prototyping machine, have been proposed.10,12,21-23 For example, Morrison et al10 designed a personalized mask that fit a child with craniofacial anomalies and found a significant decrease in air leakage from 25.2 to 6.6 L/min and a 9% increase in adherence.
The aim of this article is to provide health professionals with a comprehensive review of clinical guidelines and ergonomic methods for the design, evaluation, and personalization of NIV masks. Ergonomic considerations have been applied to the selection and use of NIV masks for safety and usability. Although ready-made NIV masks can properly support patients, NIV mask personalization would be an ideal solution to resolve the limitations of ready-made NIV masks when time is available to optimize mask interfaces to individual patients with special needs (eg, infants, patients with neuromuscular diseases and/or facial deformities). To the best of our knowledge, no reviews on NIV masks from an ergonomic perspective have been published previously.
Literature Review Methods
Ninety-three papers were screened in a systematic manner for an in-depth analysis of ergonomic issues relating to NIV mask design, evaluation, and guidelines using a 3-step process. First, 742 papers published in English within the last 10 y were identified on the Scopus and PubMed databases using the key word sets (“noninvasive ventilation” or “oxygen” or “respirator”), (“mask” or “interface”), and (“design” or “evaluation” or “development” or “customization” or “personalization”). Then, 3 reviewers independently conducted a 2-round screening by checking the titles and abstracts of the identified papers. Finally, an in-depth review was conducted after checking the full text of each of the screened papers.
Results
A total of 93 papers were selected for the in-depth review. Technical details found in the papers were summarized into 3 categories as shown in Table 1: clinical guidelines for mask selection and troubleshooting; ergonomic design issues including face anthropometry, sizing system, design tool, and design personalization; and ergonomic evaluation issues including virtual fit testing and physical fit testing.
Clinical Guidelines and Issues of Ergonomic Design and Evaluation for NIV Masks
Mask Selection
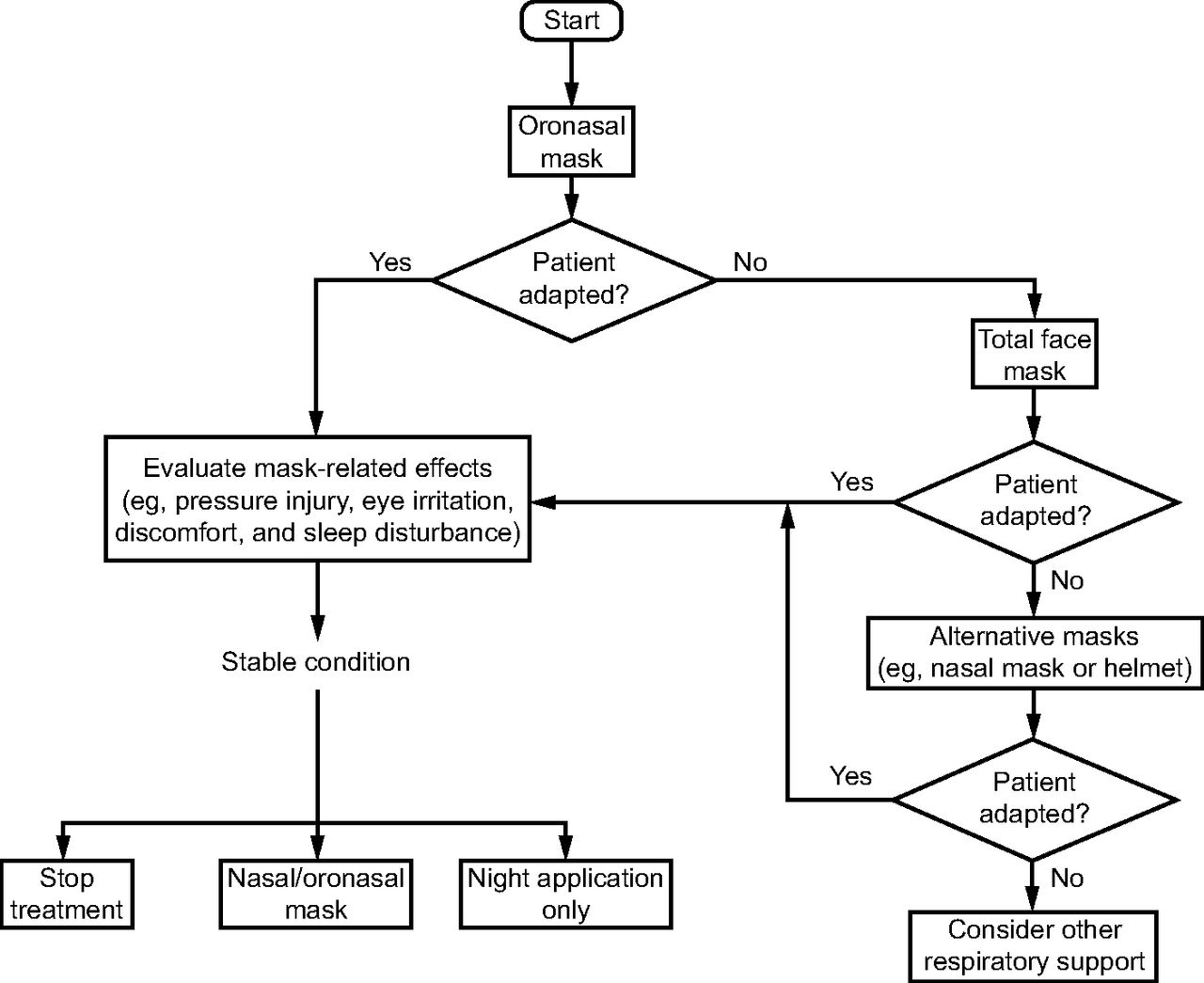
Selecting a correct mask for an NIV patient involves selecting a mask type and the correct size of the selected mask type using a size guide. Figure 2 presents the flow chart of NIV mask selection for adults and shows the initial and alternative choices of a proper mask in the clinical setting for adult patients with respiratory difficulties.4,39-40,42-43 The initial mask selection process begins with an oronasal mask and then moves to either a total face mask or a nasal mask depending on the patient’s adherence and clinical response with the mask treatment. The selection of an NIV mask in a different use context can be complex. In acute respiratory failure care, conflicting opinions exist for the initial and alternative choices of a proper mask.42 Various mask types should be available for the most appropriate mask selection because an ideal NIV interface does not exist for all patients in all circumstances.4,39 Although the oronasal mask is often selected for the initial management of acute respiratory failure with NIV42 based on literature review,4,39-41 experimental data,35-36 and survey data,37-38 the total face mask can also be the reasonable first choice.40 Other masks should be available if the patient cannot tolerate oronasal and total face masks or if complications such as facial pressure injury occur. If NIV therapy is prolonged, a switch to a nasal mask can be considered.42 The surveys37-38 in the United States and Europe provide consistent results that oronasal masks are the first choice for 70% of NIV patients followed by total face masks, nasal masks, and helmets. Note that nasal masks can be used in the beginning for some cases, but a switch to an alternative interface covering the nose and mouth is needed if air leaks occur at the mouth.35-36 Meanwhile, nasal masks are preferred for the initial management of patients with chronic respiratory failure.41 Lastly, mask selection should be completed by accommodating the patient’s opinions; however, recent studies4,42,44 reported a low level of patient involvement in the mask selection process.

The positive and negative features of various mask types are presented in Table 2, and the selection criteria for NIV masks and corresponding preferred features are listed in Table 3.6,40,44-46,48-51 Safety should be considered with the highest priority when selecting an NIV mask for minimal air leakage, minimal pressure injuries, and efficient ventilation. Pressure injuries are major concerns for patients who are totally dependent on an NIV mask for a long period of time; the status of the skin and the duration of mask wearing significantly influence the likelihood of developing pressure injuries.4,52-54 An NIV mask with a strap needs to be easy to wear, fit the face, and removable; the adaptability of an NIV mask and a strap to fit various face shapes and ventilators is an advantageous feature in NIV selection. An oronasal mask or a total face mask is suitable for patients with acute respiratory difficulties by considering ventilation efficiency, tolerance, and comfort,39-40,55 and an oral mask or a total face mask is chosen for patients with an unusual facial geometry.4 Lastly, the durability and price of NIV masks are considered to choose an affordable mask.
Criteria for Mask Selection
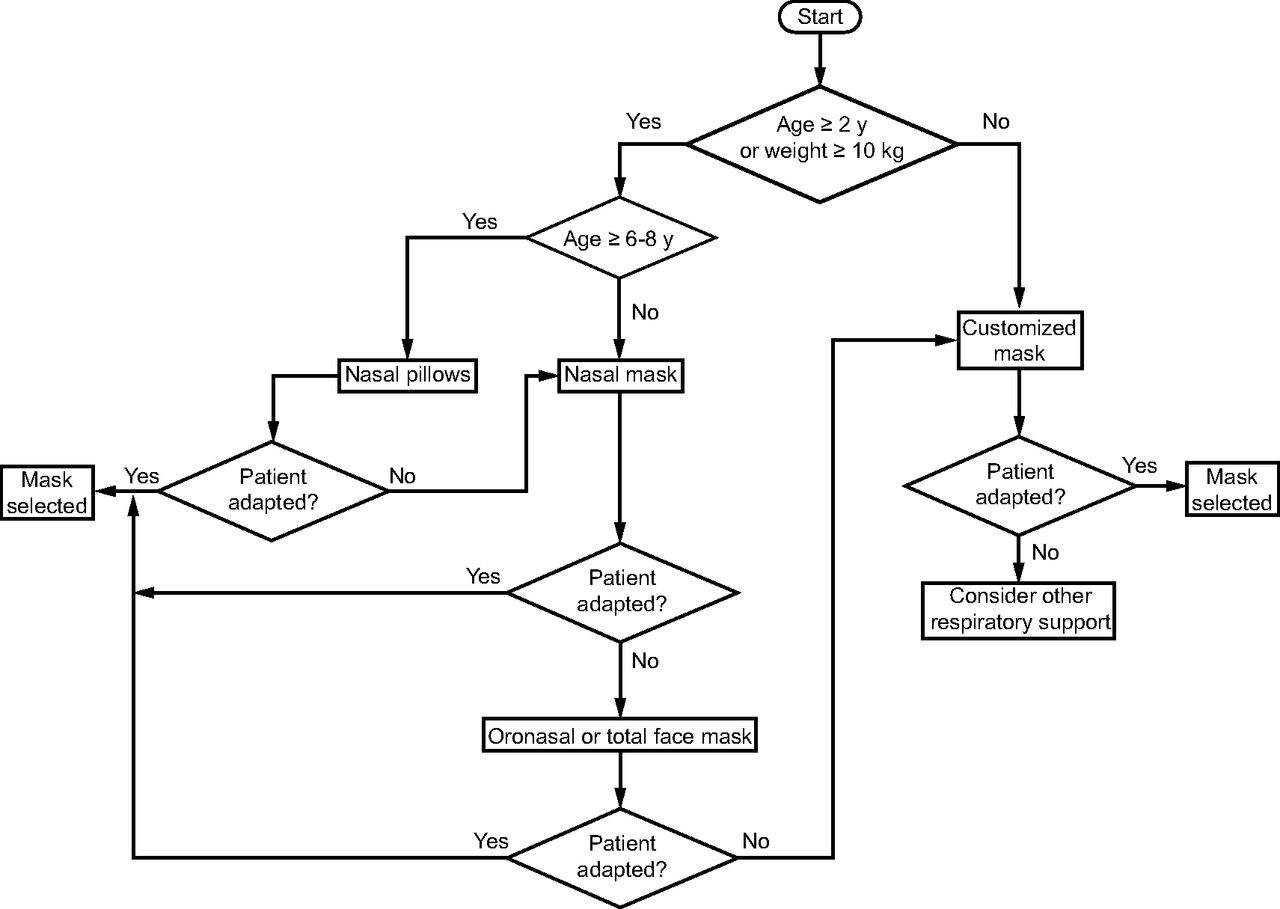
Different from masks used in adults, nasal masks are the preferred mask type for children in both chronic and acute care settings. The preference for a nasal mask can be explained by considering the risk of aspiration, problems with cooperation, learning disability, difficulty in fitting a total face mask to a child, and dead space.56 Figure 3 displays the flow chart of NIV mask selection for children in chronic settings based on the review of related papers. NIV masks for children have more requirements to minimize mask-related problems. The efficiency of a mask is more sensitive to the size and wearing location of the mask because children have smaller faces. The smallest mask should be chosen to minimize the dead space. Proper mask shape for lowest skin pressure, especially for the pressure on the maxilla, is needed to minimize cranial deformity.56 Furthermore, the weight of the mask and accessories (eg, tube, valve, circuit) should keep light to avoid dragging. Heavy accessories can drag the mask interface, which may cause usage problems for patients.6,40,48

After selecting the mask type, a sizing guide (shown in Figure 4) provided by an NIV mask manufacturer can be used to find the correct size for a patient. A customized mask can be an alternative for a patient who cannot find a mask size that fits the face and experiences significant discomfort due to the lack of fit. The time for the fabrication of a customized mask is not available for patients in acute respiratory failure.

Sizing guide for oral, nasal, and oronasal masks (adapted from sizing gauges of Philips Respironics and ResMed).
Troubleshooting When Using Masks
Table 4 summarizes the possible solutions to problems associated with NIV mask use, such as air leakage, pressure injury, nasal congestion, nasal or oral dryness, eye irritation, and claustrophobia.40,42,45,48,58-59 Most of the problems are common in long-term NIV mask users, and solutions for proper fit, strap adjustment, safe skin pressure, and monitoring have been explored. First, a proper fit of the mask to the patient’s face is achieved by a properly selected mask or custom-fabricated mask to avoid problems and side effects associated with NIV treatment.6 Second, the proper adjustment of a strap can prevent local air leakage and excessive facial contact pressure.4,40,45,60 A rule of 2 fingers beneath the strap (2-finger rule) is often used for adequate strap tension.4 Third, excessive pressure between the mask and the face can be alleviated by a nasal-forehead spacer or an adjustable forehead pad. Cushioning and barrier taping can reduce pressure injury.40,42,45,60 Lastly, regular monitoring (eg, approximately every 30 min for 6 h or up to 12 h and every h thereafter) is required.45 Rotating the types of mask used in a patient can be considered to minimize the risk of pressure injury or avoid NIV failure if the patient cannot tolerate the current mask interface or if a significant leak is detected.4,60
Problems and Solutions During NIV Mask Usage
Among the problems, pressure injury is a common adverse effect that affects both the efficacy of the NIV and the patient’s quality of life.61 In an interview of subjects with acute respiratory failure, 18% believed pressure injuries due to the mask were the worst complications they experienced.44 Pressure injury is usually a result of pressure or pressure combined with shear, localized to the skin and/or underlying tissue, over a bony prominence. Therefore, pressure injury is mainly on the nasal bridge4,40 and zygomatic bone,42 but it can develop at any part where the mask or headgear has contact with the skin. Time is another factor that influences the development of pressure injury. Carron et al58 reported that the rate of facial pressure injury (eg, erythema, ulcers) is 50% in the first few h of NIV mask use and increases to 100% after 48 h. The interventions and mask usage strategies shown in Table 4 can be applied by considering the patient’s situation. Proper strap tightness should be selected by considering the trade-off between preventing leaks and avoiding pressure injury. In addition, a mask custom fabricated to an individual’s facial contour can be provided,7 and regular assessment can be performed for the timely intervention of pressure injury.52
The use of the NIV mask in children is more problematic than that in adults because of their different physiological characteristics. Children are at greater risk of pressure injury during NIV than adults due to frequent sweating, immobility, and skin fragility.48 Moreover, they frequently need NIV for an extended period. Because of the dynamic changes in the facial contours resulting from the growth of children, the fit of the mask should be reevaluated regularly, and a switch to an alternative interface should be considered.48,57
Novel Approaches Considering Ergonomic Issues
Novel methods and solutions have been developed to resolve NIV mask problems by applying ergonomics and personalized approaches. The preferred mask design can be identified through an iterative process consisting of design refinement and testing with virtual and physical prototypes.28,62-63 It would be useful for health professionals to understand the approaches of ergonomics and personalization.
Face Anthropometry.
A set of facial dimensions and corresponding landmarks are selected in the design process of a mask. Figure 5 shows examples of facial dimensions and corresponding landmarks commonly considered in previous studies for the design and sizing system of an oronasal mask.16,64-71

Of the direct measurement, photogrammetric, and 3D-scanning methods (as shown in Table 5), the preferred method is selected by considering the advantages and disadvantages in terms of accuracy and efficiency of measurement, resource limitations, and need for postprocessing. The direct measurement method collects facial measurements using anthropometers such as calipers, tape measures, and thickness gauges. The photogrammetric method captures a photograph of the participant using a camera and then collects postmeasurements from the photo.77 The 3D-scanning method is the most sophisticated anthropometric measurement method and captures a 3D image of the body using a scanning device, prior to collecting postmeasurements as per the photogrammetric method.28,75-76,79
Mask Sizing System.
An appropriate sizing system is established for a particular type of NIV mask by considering key facial dimensions, the accommodation percentage of a user population under consideration, the level of fitting tolerance, the sizing system generation method, and the manufacturing cost constraints. A sizing system (ie, a chart of body sizes) is constructed by dividing the target population into a few categories (eg, small, medium, and large) based on key anthropometric dimensions. The key dimensions of NIV masks can differ according to the type of mask interface. Examples of key dimensions include face length and head breadth for a total face mask, face length and lip width for an oronasal mask, nose length for a nasal mask, nose width for a nasal-pillow mask, and lip width for an oral mask.17,25,28,67,80-82 Next, the target user population and its accommodation percentage of mask are determined by a business plan from the mask manufacturer, whereas the fitting tolerance of the mask is specified by considering various usability factors such as the purpose of mask usage, the material property of the mask, and the intended level of fitting comfort. Lastly, a mask-sizing system most suitable to the manufacturer is explored by adjusting the coverage of the target population by considering manufacturing costs and expected sales volumes.83-85
Process of CAD.
A mask for a particular representative face model can be designed in 3 steps: (1) initial design of the contact area, (2) refinement of the contact area, and (3) design of the remaining parts. First, the design of the contact area that fits the facial surface is initially generated based on an existing design. For example, a 3D curve contacting the face image is created by projecting a 2-dimensional contour on the 3D face model using SolidWorks (Dassault Système, Vélizy-Villacoublay, France).19-20 Next, the initial design of the contact area is refined by testing with a 3D-printed prototype or through a virtual fit method that can quantitatively analyze the fit of a mask by computer simulation.16 Lastly, the design of the remaining parts of the mask to connect to an oxygen supply system and a strapping gear of the mask to the head can be completed with a CAD tool such as Rhino 3D (Robert McNeel & Associates, Seattle, Washington) and Geomagic Freeform interconnected with a haptic device (Touch X, 3D Systems, Rock Hill, South Carolina).15,17,18,20,22
Design Personalization.
A personalized mask design is highly customized to patients in terms of fit and comfort. In some cases, it is difficult for a ready-made mask to achieve an optimized fit to the patient because of the size, shape, and design configurations (eg, vent, strap locations) of the mask for a particular face such as that of a patient with amyotrophic lateral sclerosis with facial deformities or asymmetries or a special-purpose mask for specific cohorts (eg, children). Although the customization of the NIV mask interface has not yet arrived to a wide market, many studies have proposed possible solutions to personalize NIV masks to individual patients.12,14 For example, Morrison et al10 minimized the leak and discomfort of mask usage in children with craniofacial anomalies by developing a personalized mask frame using 3D scanning, computer-aided customized design, 3D printing, and a silicone molding method. Shikama et al13 proposed a personalized adapter based on 3D solutions that can be used together with commercial masks to reduce leakage and contact pressure. In addition, semiautomatic methods added to CAD software have been proposed to help medical professionals design customized border shapes, sizes, vents, strap holes, and prepare 3D-printing models.11,21,23
Fitting Test
Virtual Fit Testing.
The adequacy of an NIV mask design for a particular group of users is evaluated in the virtual environment by investigating fit-related measures such as geometric similarity, overlapping areas, and pressure on digital face models. First, the geometric similarity between the mask’s boundary part and the face can be visually inspected by using a CAD system20 and estimated by calculating the space between the mask’s boundary and its projected contour.19 Second, the Euclidean distance between the face and mask while the mask virtually overlaps the face can be used to estimate a mask’s fit to a particular face. When locating the mask on the face, the excessive overlap between the mask and the face shows the potential chance of a poor fit.54,62 Finally, the contact pressure between the face and the mask is predicted by a finite element analysis by constructing deformable face models with mechanical properties.32,86-91 Barros et al88 and Dai et al86 built finite element face models with the anatomical structure of the face (eg, soft tissue, fat, and bone) to analyze the distribution of contract pressure, whereas Lee et al91 proposed a simplified finite element model with only the surface mesh to reduce the computational time and to utilize hundreds or thousands of 3D facial scan images in a virtual fit simulation. The virtual fit testing method can save time and cost in prototyping and usability testing and avoid a potential injury during an experiment with human subjects.54 However, a usability evaluation with human subjects using a physical prototype is required to validate the design by considering the mechanical properties of the soft tissues and the mask, the subjective feelings of the user, and the effects of medical treatment.
Physical Fit Testing.
The subjective and objective methods shown in Table 6 have been used to evaluate mask prototypes. A prototype is fabricated using 3D printing, casting, molding, or computer numerical-control machining methods by considering material, precision, time, and cost factors. In subjective evaluation, a mask prototype is evaluated in terms of comfort/discomfort, fit, leakage, and/or satisfaction for overall and/or individual regions using a Likert scale or visual analogue scale.20,63,62,89 In contrast, in objective evaluation, a mask prototype is evaluated using measurement devices for air leakage, contact pressure, and skin conditions. For air-leakage testing, a device that can measure the densities of aerosols inside and outside of a mask (eg, PortaCount Respirator Fit Tester 8038, TSI, Shoreview, Minnesota)94 or the flow of air leak (eg, BiPaP Synchrony, Philips Respironics, Murrysville, Pennsylvania).98 For contact pressure evaluation, a pressure-indicating film (eg, Prescale; Fujifilm, Tokyo, Japan)28 or a force sensor (Force Sensing Resistor; Interlink Electronics, Camarillo, California)3,13 has been used to measure the contact pressure of a mask against the face. Next, for skin condition assessment, a digital camera for checking skin redness,13,31,54 an instrument for measuring surface hydration (eg, Dermal Phase Meter 9003; NOVA Technology, Portsmouth, New Hampshire),30,54 and a biomarker for skin inflammation79,82 were used. Lastly, clinical efficacy needs to be examined using vital signs such as oxygen saturation,97 arterial blood gas analysis,92 respiratory inspiration plethysmography, 95-96 and parameters in ventilator alarm systems such as pressure and volume.93,97
Discussion
Although corrective helmets for plagiocephaly or prostheses for patients with limb amputation are widely customized using 3D scanning and 3D-printing technologies, custom NIV masks are not widely used for various reasons, including price and delivery-time factors. A poorly fitting NIV mask can cause complications including air leakage, pressure injury, ventilator insufficiency, and discomfort to patients receiving NIV treatment, which consequently leads to a need for invasive ventilation methods such as endotracheal intubation and tracheostomy. An ergonomic approach and personalization of mask designs would be a solution to NIV mask problems in the future. Various attempts10-11,99-101 have been made to individualize the mask interface for NIV treatment. Although it is generally accepted that a personalized mask is preferred to a ready-made mask in terms of safety, adherence, minimizing complications, and effectiveness, cost issues are a major concern that limits the expansion of personalized NIV masks in the clinical field. It may be important to consider prioritizing personalization for specific patient groups, including those with myopathy or chronic lung disease, who fail to apply ready-made masks during long-term use.
The ergonomic features of NIV masks summarized in the present study will be of use for health professionals to identify and prevent problems with safety and usability during NIV treatment. Selection and use guidelines for NIV masks could help health professionals to select a proper mask for an individual patient’s face and prevent problems related to mask usage. Design methods based on anthropometric data, sizing systems, and digital face models would prevent potential problems with safety and usability, such as air leakage and excessive pressure. For example, pressure injury and discomfort can be reduced by use of a customized adapter between the mask and the face, which is developed using a design technique incorporating 3D face scan data.13 Quantitative evaluation methods can help predict potential problems such as air leakage, excessive pressure, and pressure injury with high accuracy.3,9,13,20,30-31,53-54,62,89,94,102 For example, a color imaging method promises earlier detection of pressure injury than visual observation.54
For the design personalization of an NIV mask, an appropriate technology for data analysis as well as a design support system with a user-friendly interface is required. 3D-scanning technology has brought a great opportunity to design personalization, as a 3D-scan image provides the morphological information of an individual user that traditional anthropometric measurement methods cannot provide. However, 3D facial scan images have not been applied during NIV treatment because of the procedural complexity in the acquisition and editing of a 3D face scan and the optimal design of an NIV mask. A 3D face scan involves time-demanding processes such as postprocessing and landmarking for design personalization. Although recent studies38,69,74 have introduced computer technologies such as template model registration and virtual fit analysis, which can support the design of personalized products based on 3D human scan images, research is needed to shorten the process of generating a personalized mask design with a 3D face scan. Identifying a group of representative facial models that properly accommodates the target population with various face sizes and shapes, manufacturing NIV masks that properly fit to the representative face models, and recommending an NIV mask that best fits a particular patient are alternative solutions to a personalized NIV mask. Furthermore, a computerized program with a user-friendly interface needs to be developed to support health professionals to easily generate a personalized NIV mask in the clinical setting. Although personalized masks are preferable, ready-made masks are considered first in clinical practice because of economy and time limitations.4 Most personalized masks are fabricated for special conditions in which adequately fit masks cannot be found. For example, custom-made masks need to be fabricated for neonates (age < 2 y or weight ≤ 10 kg) or children who cannot adapt to a ready-made nasal prong, oronasal mask, nasal mask, or a total face mask.56 A personalized mask can be a reasonable solution for some patients as cost and time limitations are resolved in the future.
NIV has been traditionally proven to be a successful method in patients with chronic hypercapnic respiratory failure caused by a chest wall deformity, neuromuscular disease, or impaired central respiratory drive. NIV has been shown to be effective in the acute setting of COPD and cardiogenic pulmonary edema.103,104 Selecting appropriate ventilation methods for patients in acute situations is very important, and NIV should not replace invasive ventilation for those in whom NIV is not appropriate.105 From an interface point of view, both nasal and total face masks were successful for NIV in acute hypercapnic respiratory failure. Several studies comparing different types of interfaces in acute settings have not reported a strong superiority of the specific mask interface in terms of clinical efficacy.4 In the current clinical field, oronasal masks were the first choice in a large European and North American survey, followed by total face masks, nasal masks, and helmets.38
The effective dead space of the NIV masks is compared in Table 3. A large dead space was identified in the helmet and total face mask than in the oronasal mask and nasal mask, whereas the mouthpiece and lip-seal mouthpiece (oral mask) have smaller dead space. However, Fodil et al106 found that the effective dead space of the NIV interfaces was not directly related to their internal volume. The effective dead space was very close to their internal volume for the oronasal mask, whereas it reached half the tidal volume for the total face mask and the helmet regardless of the internal volume. According to Sferrazza et al,39 despite variations in internal mask volume and the effective dead space, the clinical efficacies of different masks were very similar on average. Therefore, other parameters such as comfort, synchrony, and a patient’s opinions need to be primarily considered when choosing a suitable interface for an individual patient.
Although the selection guidelines organized in the current study were organized by various empirical data sources (literature review, experimental data, and survey data), they could be limited to the number of the data, which may cause case-by-case varieties. Few studies have been conducted for NIV mask design and personalization. Various mask types in terms of oxygen mask and respirator were included in this review for NIV mask design and personalization, although they may have different pressure conditions with different face-seal requirements. The concern regarding mask selection of vented or nonvented mask type is not important from the ergonomic perspective. We focus on the shape and size of the NIV mask to the target face. Therefore, the frameworks and methodologies of other types of masks are still applicable for reference.
Summary
Further research is needed to explore better design solutions and approaches that optimize the trade-offs among the safety, usability, manufacturability, delivery time, and affordability of a mask for patients receiving NIV treatment. The personalization of a product often has a negative impact on the manufacturing simplicity, quality, delivery time, and price of a product.4,43,107 Novel solutions need to be explored and validated to provide an NIV mask with a comfortable fit for a patient in the clinical setting at an affordable price within an appropriate time frame once the facial features of the patient are identified. For example, the personalization of a mask to the patient can be conducted at the end of the NIV mask supply chain by applying a novel solution to product architecture and modularization while maintaining reasonable mask delivery times and prices.
Footnotes
- Correspondence: Sungchul Huh MSc, Department of Rehabilitation Medicine, Pusan National University Yangsan Hospital, 20 Geumo-ro, Mulguem, Yangsan, Gyeongnam 50612, Republic of Korea. E-mail: dr.huhsc{at}gmail.com
The authors have disclosed no conflicts of interest.
This study was supported by the Research Institute for Convergence of Biomedical Science and Technology, Pusan National University Yangsan Hospital.
- Copyright © 2022 by Daedalus Enterprises
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.
- 27.
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.
- 48.↵
- 49.
- 50.
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.
- 66.
- 67.↵
- 68.
- 69.↵
- 70.
- 71.↵
- 72.↵
- 73.
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.
- 79.↵
- 80.↵
- 81.
- 82.↵
- 83.↵
- 84.
- 85.↵
- 86.↵
- 87.
- 88.↵
- 89.↵
- 90.
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}